Infective endocarditis is a condition which occurs in the setting of bacteraemia whereby endothelial surfaces of the heart, such as valvular structures, become infected. It can present acutely or subacutely, and is often associated with fevers, new heart murmurs, constitutional symptoms and embolic phenomena. The classical organism associated is Staphylcoccus aureus, however there are many other organisms which can cause infective endocarditis. This is particularly dependent on the presence of native or prosthetic valves, history of intravenous drug use and recent cardiac surgery.
Definition
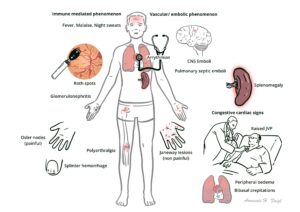
Infective endocarditis: A microbial process of the endocardium, usually involving the heart valves Janeway lesions: Painless hemorrhagic macules on the palms and soles that are consistent with infectious endocarditis, thought to be caused by septicemboli, resulting in microabscesses Osler Node: Painful, palpable, erythematous lesions most often involving the pads of the fingers and toes, they represent vasculitic lesions caused by immune complexes. Roth spots: Hemorrhagic retinal lesions with white centers, due to infectious endocarditis, also thought to be an immune-complex–mediated vasculitis.
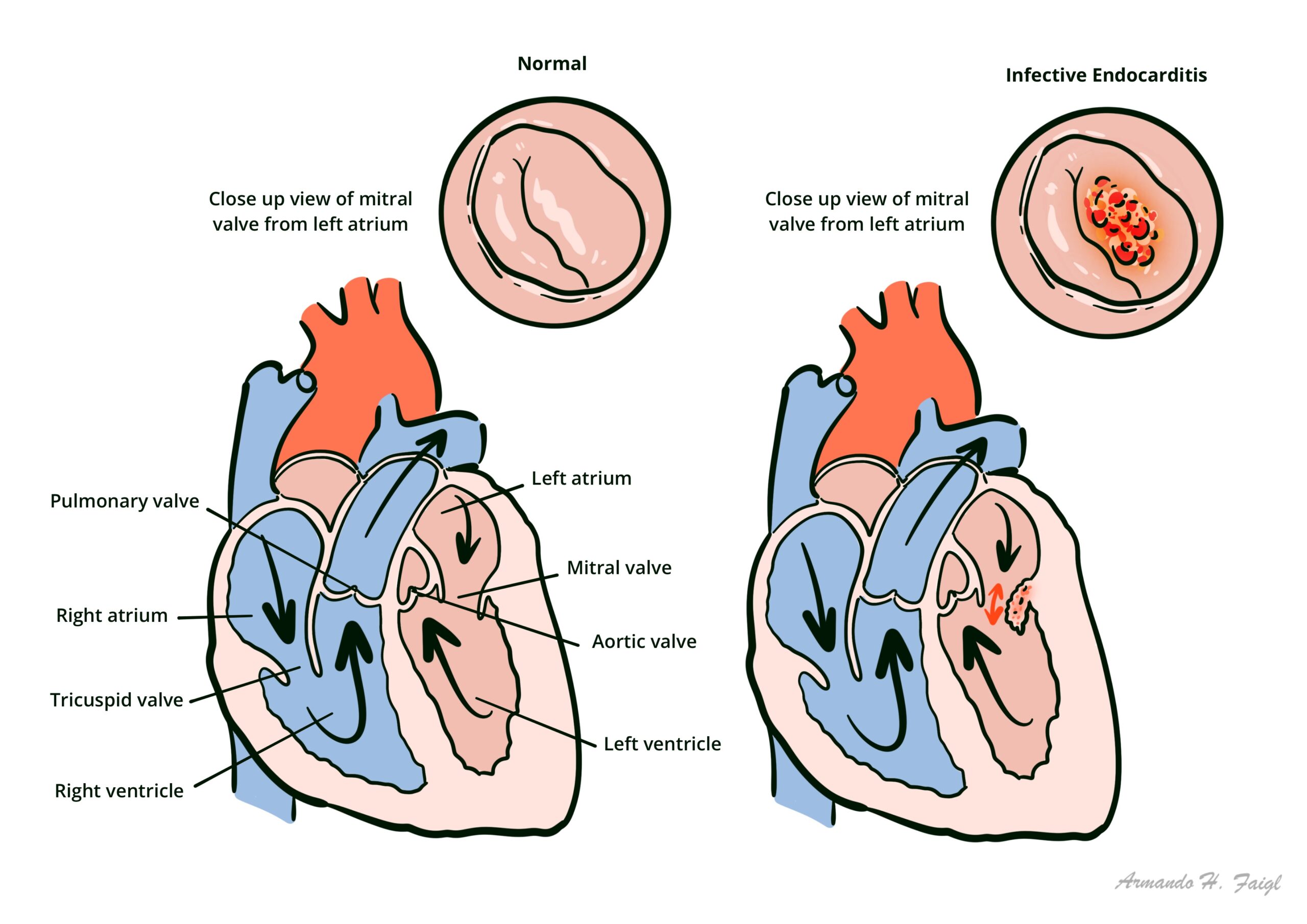
Turbulent blood flow across valvular surfaces can lead to endothelial damage which acts as substrate for platelets and fibrin to adhere. In the setting of bacteraemia, these areas become colonised which perpetuate further deposition of fibrin and platelets. This ultimately leads to vegetation formation which can produce new heart murmurs from regurgitant valves. In addition, it can cause distal embolic phenomena.
Cardiac valves involved: Mitral valve > aortic valve > tricuspid valve > pulmonary valve (except for IVDU, in which case 50% of cases affect tricuspid valve)
Depending on patient risk factors, there are a number of organisms which can cause infective endocarditis (above). There are several clinical patterns which can help predict the organism associated:
Native valve involvement
Absent IVDU – Staphylcocci, Enterococci, Streptococci viridans group
With IVDU (often right sided involvement) – Staphylcocci, Streptococci, gram negative bacilli, polymicrobial infections
Vegetation on heart valves are the classic hallmarks of infective endocarditis. The vegetations are friable, bulky, potentially destructive les
Clinical Manifestation
Infective Endocarditis presents with non-specific signs and symptoms. Highly variable presentation—depends on intracardiac pathology, virulence of organism, and extracardiac involvement. Only a small proportion of people actually present with the risk factors mentioned above.
Diagnostic criteria – Duke criteria for IE – Must meet 2 major criteria or 1 major and 3 minor criteria or 5 minor criteria.
Major criteria:
Positive blood culture for infective endocarditis (IE):
Typical micro-organism for IE from 2 separate blood cultures
Persistently positive blood cultures.
Evidence of endocardial involvement:
Oscillating intracardiac mass on valve/supporting structures, or in the path of regurgitant jet in the absence of an alternative anatomical explanation
Abscess
New partial dehiscence of prosthetic valve or new valvular regurgitation.
Minor criteria:
Predisposing heart condition or intravenous drug use
Fever over 38°C (>100.4°F)
Vascular phenomenon such as major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhage, Janeway lesions
Most commonly required for refractory congestive cardiac failure
Also indicated in valvular ring abscess, fungal causes, valvular perforation, ≥2 major emboli, antimicrobial failure, mycotic aneurysms, or staphylococcus infection of prosthetic valve



















Discussion