

Hypercholesterolaemia
Overview
Higher levels of cholesterol associated with worse CV outcomes. Three main types that are measured: VLDL, LDL and HDL. High LDL is associated with a significant increase in cardiovascular problems. Hypercholesterolaemia can also run in families. Lifestyle modification aim to reduce cardiovascular risk. Pharmacological agents are lipid lowering drugs, statins being first-line.
Lipid Physiology
Four main lipoproteins in our body and their general function:
- Cholymicrons – transporting lipids from the GIT to many organs and finally the liver
- VLDL – Triglyceride transporter
- LDL – cholesterol transporter
- HDL – picking up excess cholesterol
Chylomicrons: Assembled in mucosal epithelial cells in small intestine. Required for transport of dietary lipids to adipose tissue for storage. Made up predominately of triglycerides.
VLDL: Transports triglycerides made in hepatocytes to adipocytes for storage. Converted to LDL after depositing triglycerides. Contains predominately triglycerides
LDL: Carry about 75% of total cholesterol in blood and delivers to cell membranes and synthesis of steroid hormones and bile salts. Contains apo B100 which binds LDL receptors allowing endocytosis and breaking down to serve cellular needs. There is negative feedback inhibiting synthesis of new LDL receptors once cell has sufficient cholesterol. Predominately made up of cholesterol.
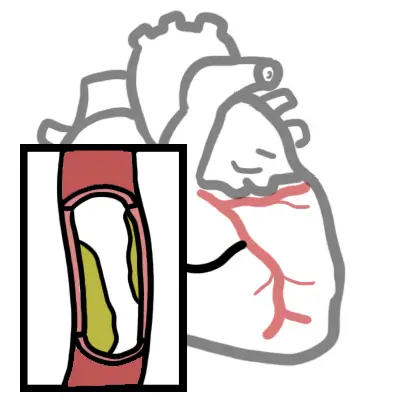
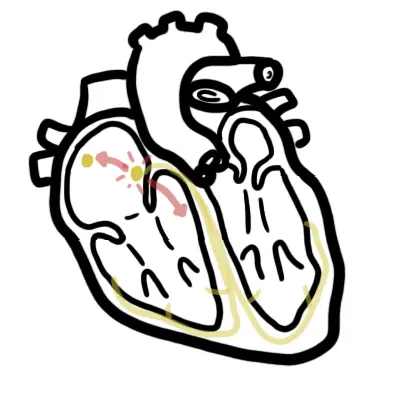
- In excess – Deposition in/around smooth muscle fibres in arteries → Fibrofatty plaques in atherosclerosis
HDL: Made in the liver and removes excess cholesterol from body cells and blood and delivers to liver for elimination. Contains 40-45% protein, 30% phospholipid, 20% cholesterol, 5-10% triglyceride.
Aetiology & Risk Factors
Aetiology
Hyperlipidaemia is considered to be the presence of an abnormal lipid profile, typically involving predominant hyperglyceridaemia, hypercholesterolaemia or a mixed pattern of both. It is commonly attributed to primary causes or due to high fat diet and sedentary lifestyle, however other secondary causes need consideration.
Primary (affecting lipid metabolism directly)
Secondary dyslipidaemia
- Renal failure
- Nephrotic syndrome
- Hypercholesterolemia
- Hypothyroidism
- Pregnancy
- Cholestatic disease
- Alcohol Abuse
- Drugs
- Ani-retroviral proteases inhibitors
- Thiazides
- Oral contraceptive pill
- Steroids
- Insulin Resistance
- Excess body weight
- Hypothyroidism
- Cholestatic liver disease
- Smoking
- Nephrotic syndrome
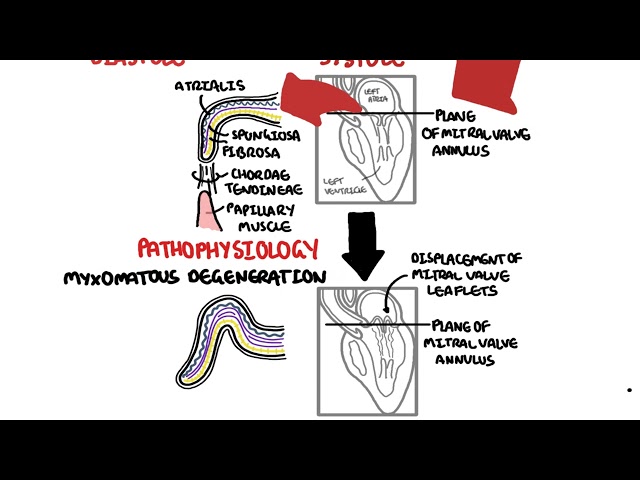
Pathophysiology
Clinical Manifestation
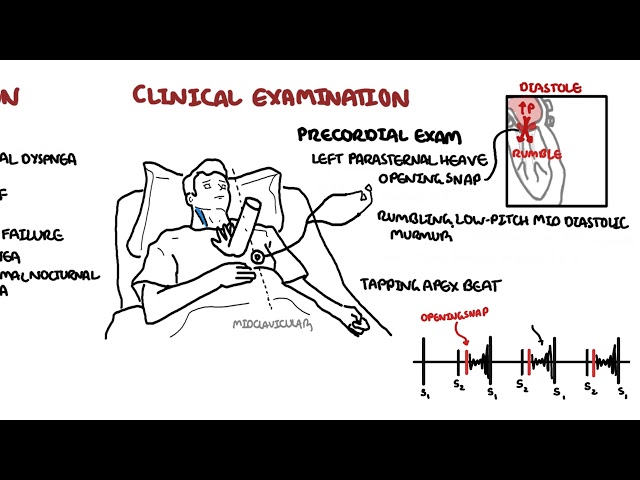
Clinical Examination
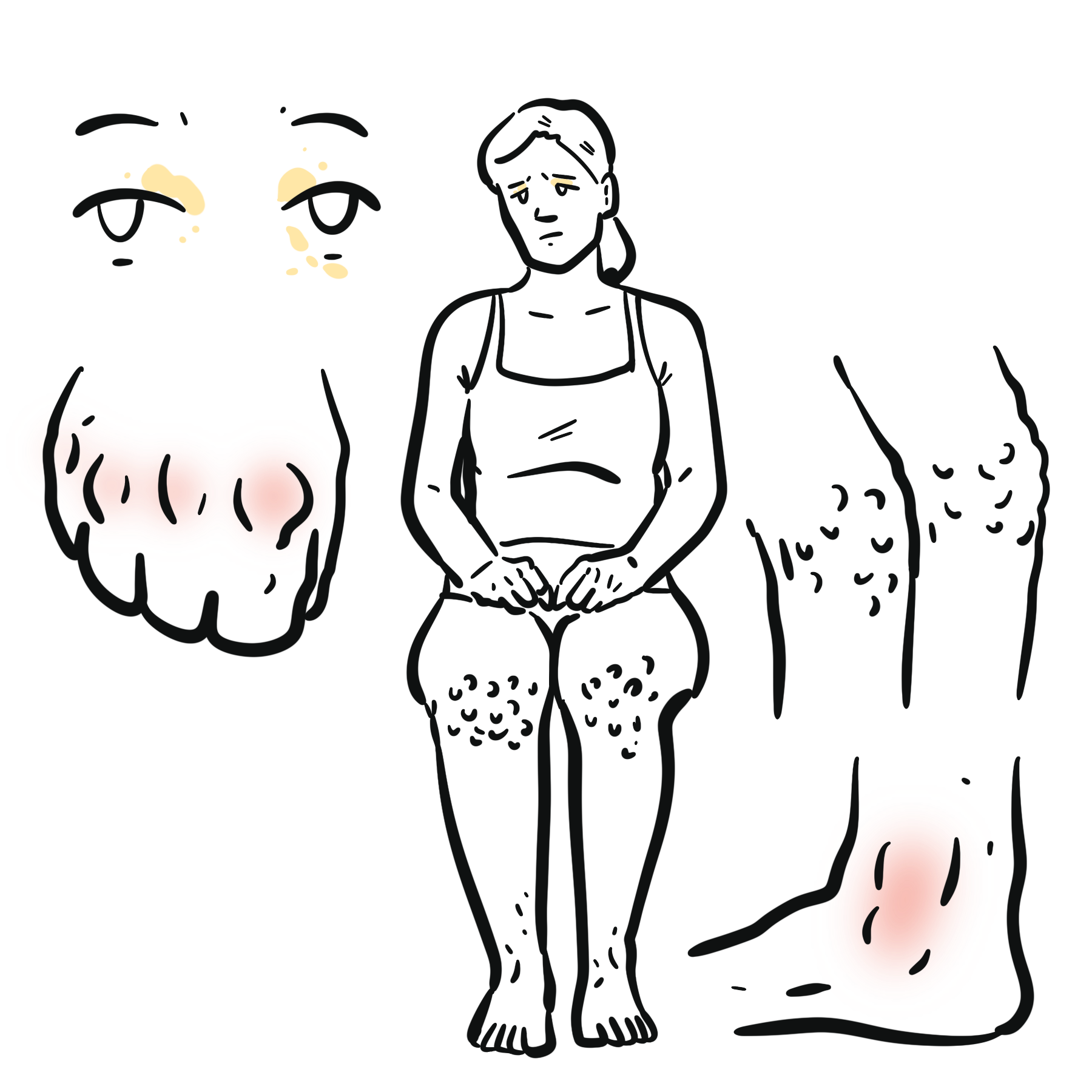
- Overweight/obese
- Xanthelasmas
- Tendinous xanthomas (xanthomata)
- Corneal Arcus: A hazy, grey or white ring that forms around the colored part (iris) of the eye.
- Lipemia Retinalis: A creamy, pale appearance of the blood vessels in the retina, typically seen in severe hypertriglyceridaemia.
- Obstructive liver disease
- Nephrotic Syndrome
- Chronic Kidney Disease
- Hypothyroidism
- Anorexia nervosa (increased triglycerides and/or decreased HDL)
- Chronic alcohol use OR oestrogen use (increased triglycerides and HDL may increase rather than decrease)
Investigations
- Lipid Profile (fasting)
- Non-fasting
The following parameters are assessed:
- Total cholesterol
- HDL cholesterol
- LDL cholesterol
- Triglycerides
Only the total cholesterol and high-density lipoprotein cholesterol (HDL-C) levels are required to calculate absolute CVD risk. Not LDL like one would think.
| Normal ranges for plasma lipid levels | |
| Total Cholesterol | 4.0-6.5 mmol/L |
| LDL cholesterol | <4.1 mmol/L |
| HDL cholesterol | 0.8 – 2.0 mmol/L |
| Triglycerides | 0.8-2.0 mmol/L |
Treatment
| Target plasma lipid levels for patients on lipid-modifying therapy | |
| Total cholesterol | <4.0 mmol/L |
| LDL cholesterol | <2.0 mmol/L |
| HDL cholesterol | >1.0 mmol/L |
| Triglycerides | <2.0 mmol/L |
Non-pharmacological (Life-style modicfication)
- Dietary changes – Reducing saturated and trans fats, increasing soluble fibre, replacing saturated fats with monounsaturated and polyunsaturated fats, introducing plant sterol enriched milk, margarine or cheese products (most effective)
- Reduce alcohol intake
- Encourage weight loss (if overweight or obese)
- Encourage physical activity
Follow up every 12 months
Most effective strategy to increase HDL cholesterol levels is to reduce weight and exercise.
Pharmacological
- Statin (first-line)
- Ezetimibe
- Bile acid binding resins
- Nicotinic Acid
- Fibrates – reduce LDL cholesterol by 5-10%. Major effects also to lower triglycerides by 35-50% and raise HDL cholesterol by 5-20%.
Adverse effects of lipid-modifying therapy include liver dysfunction and muscle problems. Alanine aminotransferase [ALT] and creatine kinase [CK] should be tested at baseline and when the response of lipids is assessed (1 to 2 months after initiation or dosage adjustment).
Pharmacology
Statins is a competitive HMG-CoA reductase inhibitor, an enzyme responsible for producing cholesterol. By lowering the levels, they help prevent heart attacks and stroke. Side effects: Headache, difficulty sleeping, flushing of the skin, myalgia, liver enzyme dysfunction, nausea or vomiting, abdominal cramping or pain, bloating or gas and serious cases myositis and Rhabdomyolysis.
Pharmacology
Ezetimbe inhibits absorption of cholesterol at brush border of small intestine via NPC1L1 transporter. Reduces cholesterol delivery to liver, reduces hepatic cholesterol stores and increases clearance of cholesterol. Side effects: Fatigue, diarrhoea, hepatic dysfunction, arthralgia, URTI, sinusitis, influenza.
Management in the Elderly
Non-pharmacological
- Dietary changes
- Reduce alcohol intake
- Encourage weight loss (if overweight or obese)
- Encourage physical activity
Pharmacological
In the elderly, statin therapy has weak evidence due to the natural increase in cardiovascular risk with age, as well as adverse effects which contribute to morbidity and mortality. In general, statin therapy should be discontinued or exempted when there is no clinical benefit of treatment or risks are greater than any potential benefit.
Complications & Prognosis
- ↑↑Ischaemic Heart Disease Risk
Cardiovascular risk assessment should be performed every 2 years for ≥45 year olds who do not have cardiovascular disease and are not determined to be at high risk (diabetes or with microalbuminuria, moderate or severe CKD, SBP ≥180mmHg/DBP ≥110mmHg, total cholesterol ≥7.5).
Familial hypercholesterolaemia
Familial hypercholesterolaemia is a dominantly inherited condition that affects over 1 in 500 people and accelerates cardiovascular disease by 20 to 40 years.
It should be considered in patients with severely elevated LDL, or those with tendon xanthomata or a strong family history of premature cardiovascular events.
- ↑risk of acute coronary syndrome
- ↑risk of cerebrovascular events
References
UpToDate
BestPractice





Members only discussions coming soon…