

Atrial Fibrillation
Overview
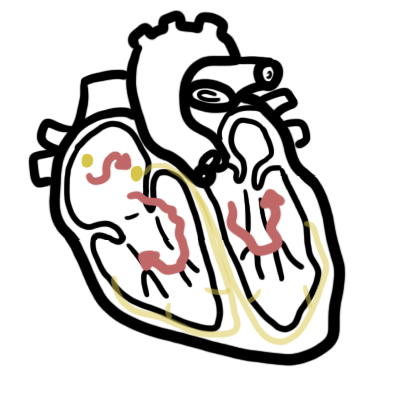
Atrial fibrillation, AF is a chaotic, irregular atrial rhythm at 300-600bpm; the AV node responds intermittently, hence an irregular ventricular rate. AF is the most common sustained dysrhythmia; characterised by absent P waves, irregularly irregular heart rate, narrow QRS (typically). It is common in the elderly. The main risk of AF is embolic stroke either in the mesenteric artery, brain tissue or limb extremities.
Definition
Supraventricular tachyarrhythmia: Arrhythmia arising from the conduction system above the ventricles, possibly the AV node, atria or SA node.
Atrial Fibrillation: A supraventricular tachyarrhythmia. It is characterised by uncoordinated atrial activity on the surface ECG, with fibrillatory waves of varying shapes, amplitudes, and timing associated with an irregularly irregular ventricular response when atrioventricular (AV) conduction is intact.
Acute Atrial Fibrillation: Defined as a new onset or a first detectable episode of AF, whether symptomatic or not.
Chronic Atrial Fibrillation: is defined as experiencing atrial fibrillation more than once. It may be paroxysmal, persistent, long-standing persistent, or permanent.
Anatomy & Physiology
The cardiomyocytes contract moving blood around and out of the heart. Many factors affect cardiac output, one of which is heart rate.
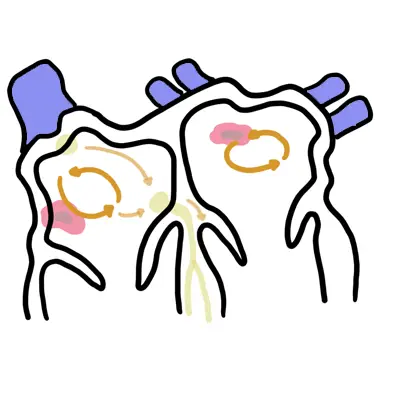
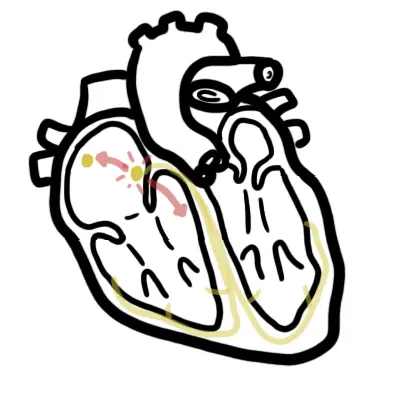
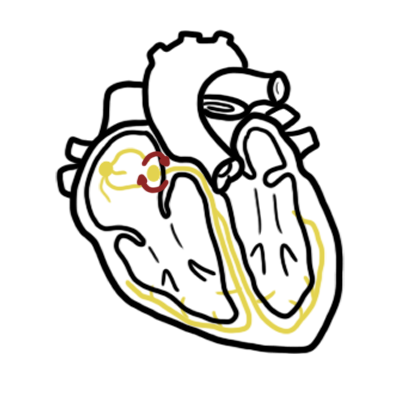
Conduction system The heart rate is controlled by the heart’s own special conduction system. The Sino atrial node (SAN) is the boss and sits high in the lateral right atrium (RA) just below the superior vena cava. The SAN is richly innervated with sympathetic and parasympathetic fibres, which alter the rate of depolarization hence controlling the heart rate. This is also the same for the Atrioventricular node which is found in the RA anterior to the mouth of the coronary sinus and directly above the insertion of the septal leaflet of the tricuspid valve. The AV node then sends conduction signals to down to the ventricles through the his-purkinje system.
Aetiology & Risk Factors
- Heart Failure
- Hypertension
- Post MI
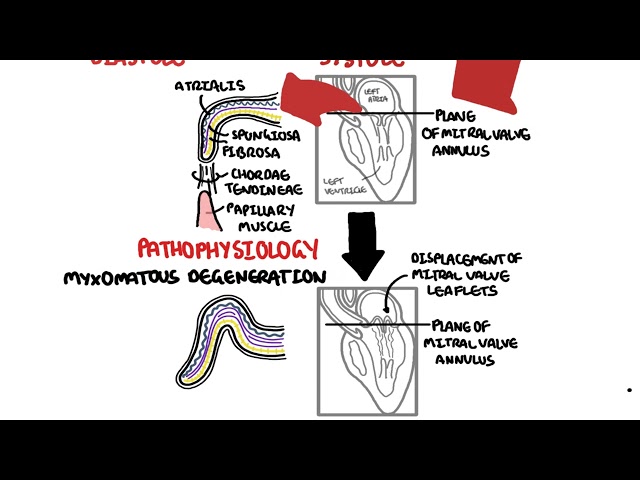
- Mitral Valve disease
- Hyperthyroidism
- Post-Op
- HOCM
Classification
Three clinical patterns (3Ps) All patterns have a risk of thromboembolism.
- Paroxysmal AF: Defined as recurrent and terminates spontaneously within 24hours -48 without any intervention
- Persistent AF: Defined as AF that is sustained >7 days or lasts <7 days but necessitates pharmacological or electrical cardioversion
- Permanent (Chronic) AF: refractory to cardioversion or accepted as a final rhythm. A decision has been made not to pursue restoration of sinus rhythm by any means, including catheter or surgical ablation
Chronic AF is having atrial fibrillation more than once. It may be paroxysmal, persistent, long-standing persistent, or permanent.
Clinical Manifestation
Clinical Presentation
Atrial fibrillation may cause chest pain, palpitations, dyspnea, or faintness. Signs include irregularly irregular pulse and possible signs of left ventricular heart failure. 30% of patients present with AF as an incidental finding only
AF may be associated with non-cardiac disease (ie. pneumonia and hyperthyroidism).
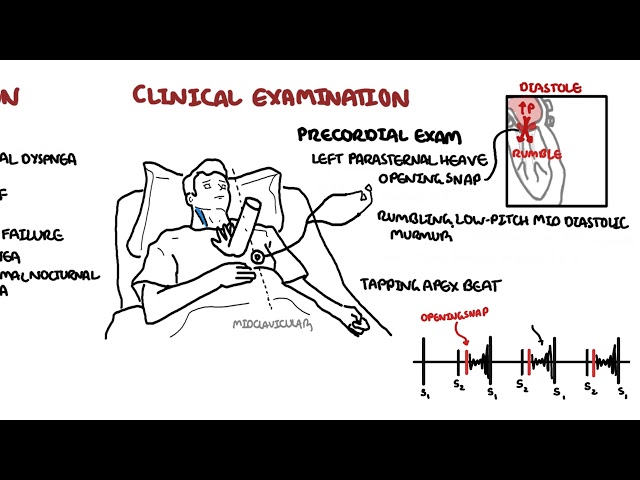
Examination
- Irregular pulse (which if rapid will be faster at the apex than the wrist)
- Variable intensity of the first heart sound
- Absent ‘a’ waves in the JVP
Palpitations
- Chronic atrial fibrillation
- Paroxysmal atrial tachycardia
- Atrial flutter
- Wolff-Parkinson-White syndrome
Wolff-Parkinson-White syndrome is a condition in which there is an extra electrical pathway in the heart (accessroy pathway). The condition can lead to periods of tachycardia.
Investigations
- ECG – changes in AF or MI
ECG shows absent p waves, irregularly irregular rhythm, QRS (typically narrowed). Rate is usually about 150bpm
- Echocardiogram – valvular heart disease
- Chest x-ray – heart failure
- Troponin – MI?
- ABG – if shocked, hypoxic or signs of acidosis
- For non-cardiac causes
- Thyroid function test
- Full blood count – ↑WCC (pneumonia)
- EUC – hypokalaemia +/- renal impairment
- Other investigations when the patient is stable
- 24-hour ambulatory monitor to assess heart-rate control and look for episodes of symptomatic bradycardia
- Exercise test (or other ischaemia stress test)
- Coronary angiography
- Cardiac magnetic resonance.
Treatment
The treatment of atrial fibrillation needs to be considered under three seperate headings:
- Diagnose AF stable or unstable?
- If unstable – Cardioversion
- Rate control
- Rhythm control
- Thromboembolic disease prevention
Haemodynamically unstable AF
- ABCD
- Correct underlying electrolyte imbalance
- ECG
- Emergency cardioversion – if unstable AF
- Electrical – 100 joules
- Chemical – Amiodarone OR flecinide
- Identify underlying cause
- Treat underlying cause
Acute AF but haemodynamically stable
- Either Rate control or Rhythm control
- Rate Control – Betablocker or CCB or Digoxin
- Digoxin good in Heart failure
- Consider elective cardioversion
- Tranoesophageal ultrasound before cardioversion to prevent thromboembolism from atrial ‘stunning’ OR
- Start anticoagulants for 3weeks to reduce risk of thromboembolism
- Heparin bridging for Warfarin (INR 2-3) OR
- NOAC – Dapigatran (Factor IIa inhibitor)
- Maintenance therapy after cardioversion or after AF has revereted
- Rhythm control – flecanide OR sotalol OR amiodarone (most effective but crazy side effects)
- no need for antiarrythmic if AF is associated with a transient condition
- Assess risk for embolus using (CHADSVASc SCORE)
- If low emboli risk – stop anticoagulant if sinus rhythm normal and risk of emboli is low.
- If moderate – high emboli risk start prophylaxis
- Aspirin
- Warfarin (INR 2-3) OR NOAC – dapigatran
- Rhythm control – flecanide OR sotalol OR amiodarone (most effective but crazy side effects)
Chronic AF – ongoing management
- Rate Control – Betablocker or CCB or Digoxin
- Anticoagulation
- Warfarin OR
- NOAC
- Rhythm Control – Sotalol or Amiodarone
- Catheter or surgical ablation if rate and rhythm control ineffective
Warfarin (international normalized ratio (INR) >2) reduces strokes in AF by 60%, regardless of underlying risk.
| CHADS2 Scoring system to assess risk of stroke in AF (nonvalvular) | |
| 1 point each | 2 point each |
| Congestive Heart Failure | Stroke or TIA previously |
| Hypertension | |
| Age >75yo | |
| Diabetes | |
| CHA2DS2 – VASc Scoring system to assess risk of stroke in AF (nonvalvular) | |
| 1 point each | 2 point each |
| Congestive Heart Failure | V |
| Hypertension | Age >75 |
| Age >65yo | Stroke or TIA previously |
| Diabetes | c |
| Sex – female | |
| Vascular disease | |
Pharmacology
Warfarin is an anticoagulant. It is used for AF, valvular heart disease and pulmonary embolism. Mechanism of action: Vitamin K antagonist inhibiting the production of coagulation factors VII, IX, X (these require Vitamin K to be produced). Side effects: Allergy, acute bleeding. When bleeding occurs as a result of warfarin this can be reversed by administering Vitamin K.
Pharmacology
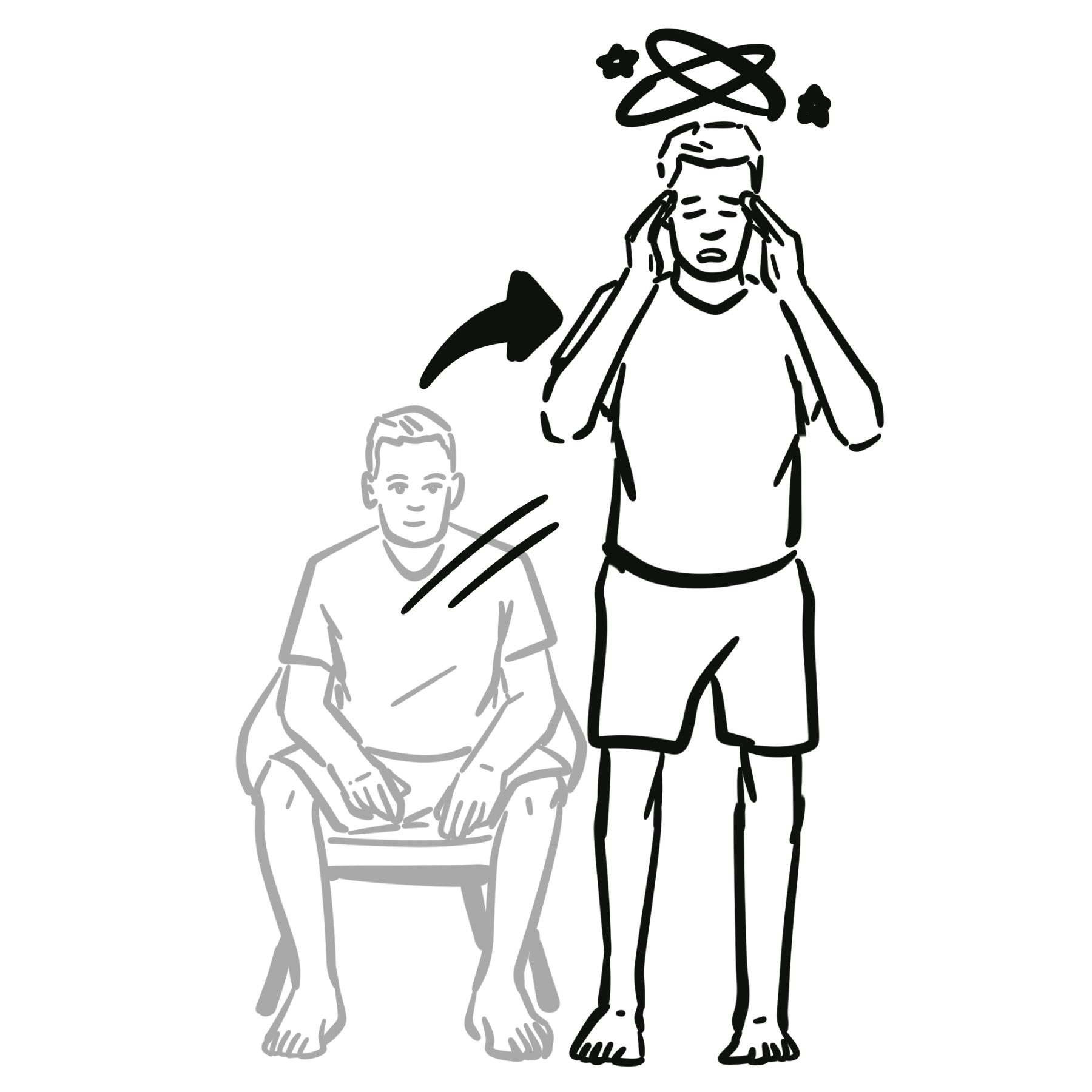
Digoxin is used for Heart failure and AF. Digoxin works by inhibiting the Na/K+ pump in cardiomyoctyes, this causes ↑intracellular Na+ together with Ca+ causes stronger contractions at a slower rate. Side effects: Nausea, vomiting, headache, dizziness/vertigo, loss of appetite, diarrhea, Digoxin toxicity (arrythmias).
Pharmacology
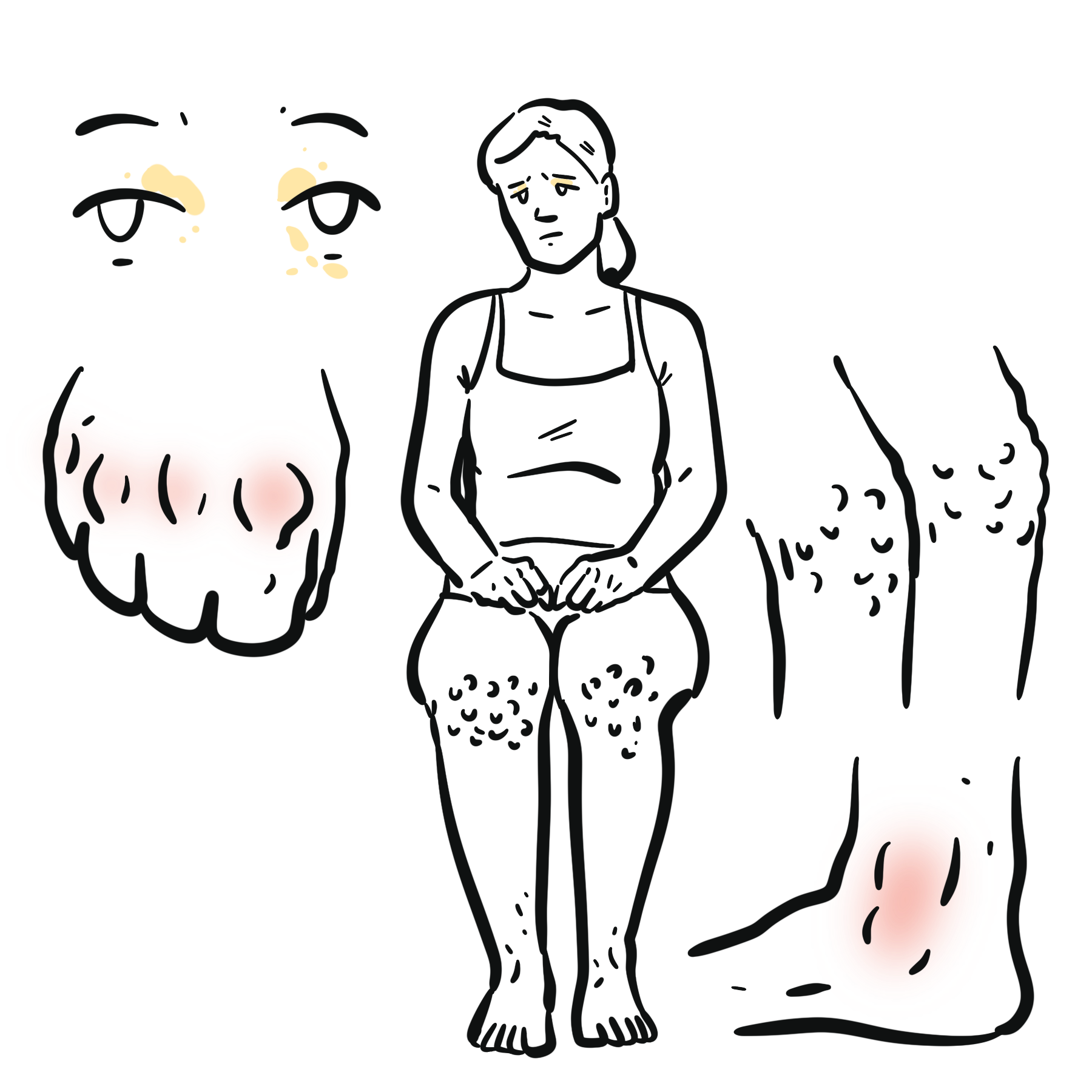
Amiodarone is a K+ channel blocker (class III antiarrythmic). It acts on the myocardium to delay repolarization and increase duration of the action potential. It also decreases SA and AV conduction rate. Side effects (6Ps): Prolongs action potential duration, Photosensitivity, Pulmonary fibrosis and inflammation, Pigmentation of skin, Peripheral neuropathy, Peripheral conversion of T4 to T3 is inhibited (Hypothyroidism, but it also can cause hyperthyroidism).
Complications & Prognosis
- Death
- Bradycardia
- Stroke
- Heart failure
- Hypotension
- Amiodarone toxicity
- Pulmonary Inflammation +/- Fibrosis
- Thyroid Dysfunction
6Ps of Amiodarone side effects (6Ps): Prolongs action potential duration, Photosensitivity, Pulmonary fibrosis and inflammation, Pigmentation of skin, Peripheral neuropathy, Peripheral conversion of T4 to T3 is inhibited (Hypothyroidism).
Prognosis depends on several factors, such as the precipitating event, underlying cardiac status, risk of thromboembolism, and whether the nature of the AF is paroxysmal, persistent, or permanent.
References
UpToDate
Best Practice
Oxford Handbook of Cardiology






Members only discussions coming soon…