

Pericarditis
Overview
Pericarditis is the most common form of pericardial disease and a relatively common cause of chest pain. The etiology of pericarditis may be infectious (eg, viral and bacterial) or noninfectious (eg, systemic inflammatory diseases, cancer, and post-cardiac injury syndromes). Tuberculosis is a major cause of pericarditis in developing countries but accounts for less than 5% of cases in developed countries, where idiopathic, presumed viral causes are responsible for 80% to 90% of cases. The diagnosis is based on clinical criteria including chest pain, a pericardial rub, electrocardiographic changes, and pericardial effusion.
Definition
Acute pericarditis: An inflammation of the pericardial sac surrounding the heart.
Pericardial friction rub: Harsh, high-pitched, scratchy sound, with variable intensity, usually best heard at the left sternal border by auscultation, due to pericarditis.
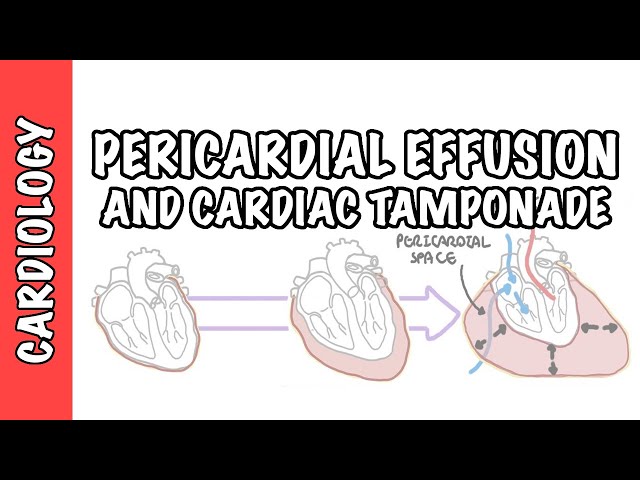
Pericardial Effusion: Fluid that fills the pericardial space, which may be due to infection, haemorrhage, or malignancy. A rapidly accumulating effusion may lead to cardiac compromise.
Cardiac Tamponade: Increased pressure within the pericardial space caused by an accumulating effusion, which compresses the heart and impedes diastolic filling.
Anatomy of the Pericardium
The pericardium is a membranous layer that covers the heart and helps protect it, fixes the heart in the mediastinum and lubricates the heart.
The pericardium has two layers:
The pericardium has two layers:
- The serous pericardium has a parietal and visceral layer and forms a closed sac
- The parietal layer lines the inner surface of the fibrous pericardium and is reflected onto the heart as the visceral layer, or epicardium
- Between the parietal and visceral pericardium is the pericardial space which contains serous fluid, important in
- The fibrous pericardium is the outermost layer, and it is firmly bound to the central tendon of the diaphragm.
Aetiology and Risk Factors
Aetiology
- Idiopathic or presumed viral infection
- Post-myocardial infarction pericarditis
- Following cardiac surgery or cardiac procedures
- Autoimmune disease:
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Systemic sclerosis
- Autoinflammatory disorders
- Malignancy
- Advanced kidney failure—uraemic pericarditis
- Chest trauma
- Radiotherapy
- Medication-induced pericarditis.
Important infectious causes
- Viral infection
- Tuberculosis
- Bacterial or purulent infection
- Fungal or parasitic infection, particularly in immunocompromised patients
Pathophysiology
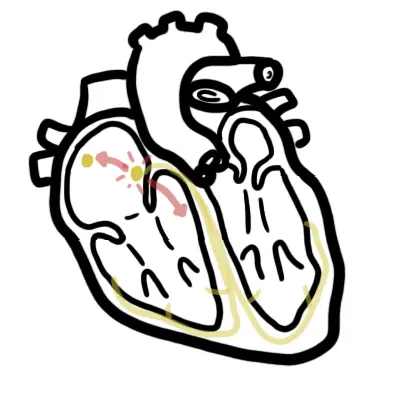
- Infection, autoimmune activation, tissue injury or another trigger causes inflammation of the pericardial layers.
- Inflamed layers rub against each other, producing pleuritic chest pain and a pericardial friction rub.
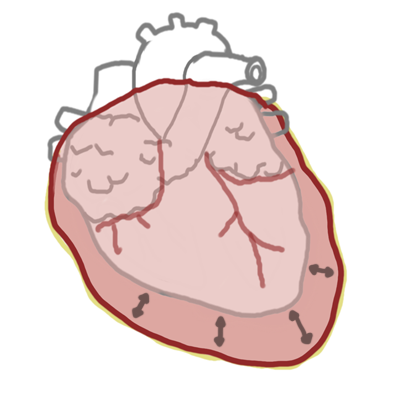
- Inflammation may increase pericardial fluid production, causing an effusion.
- Rapid or large fluid accumulation can impair ventricular filling and cause cardiac tamponade.
- Persistent inflammation may cause fibrosis, thickening and loss of pericardial elasticity, resulting in constrictive pericarditis.
- Immune-mediated inflammation is important in idiopathic and recurrent pericarditis, including activation of the interleukin-1 pathway.
Clinical Manifestations
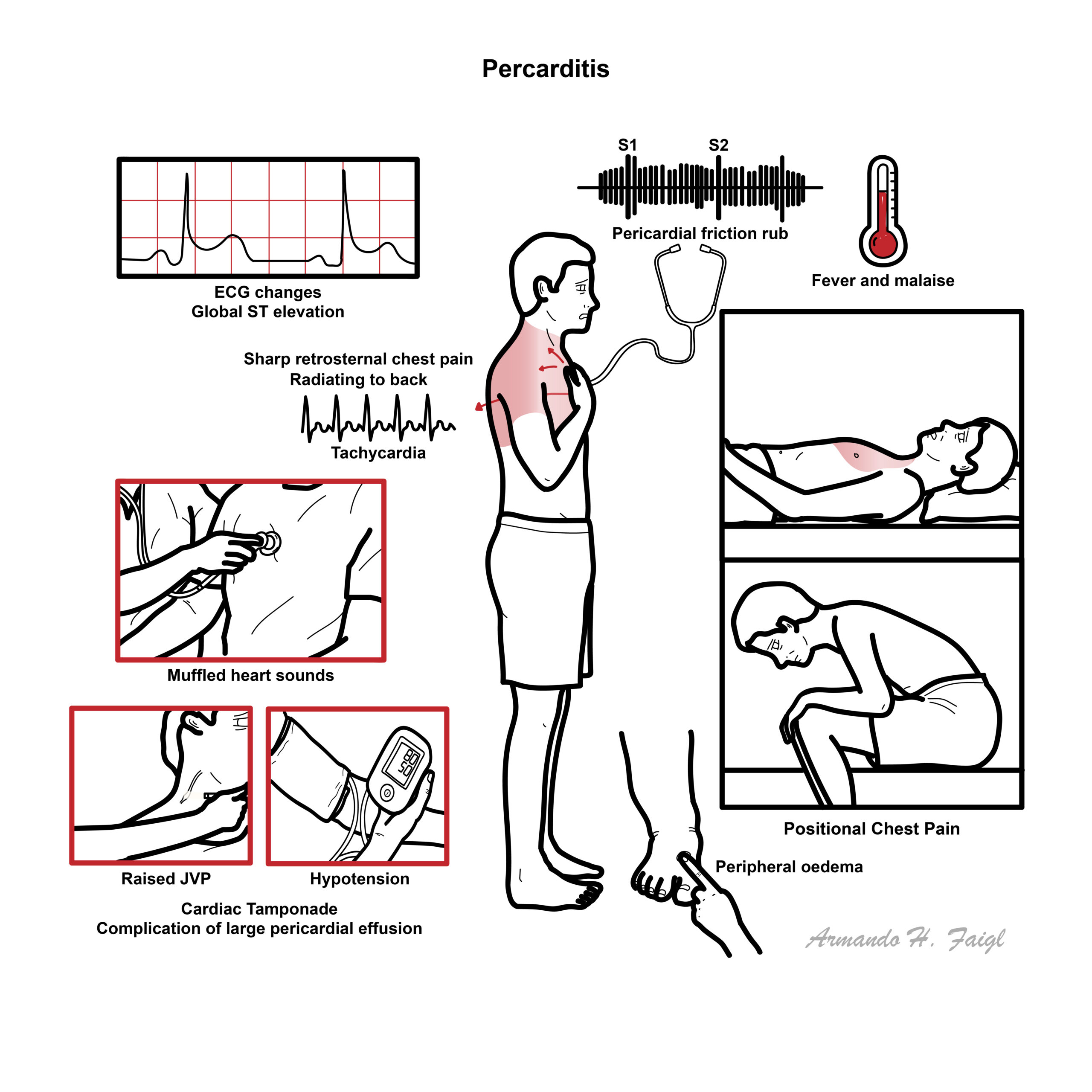
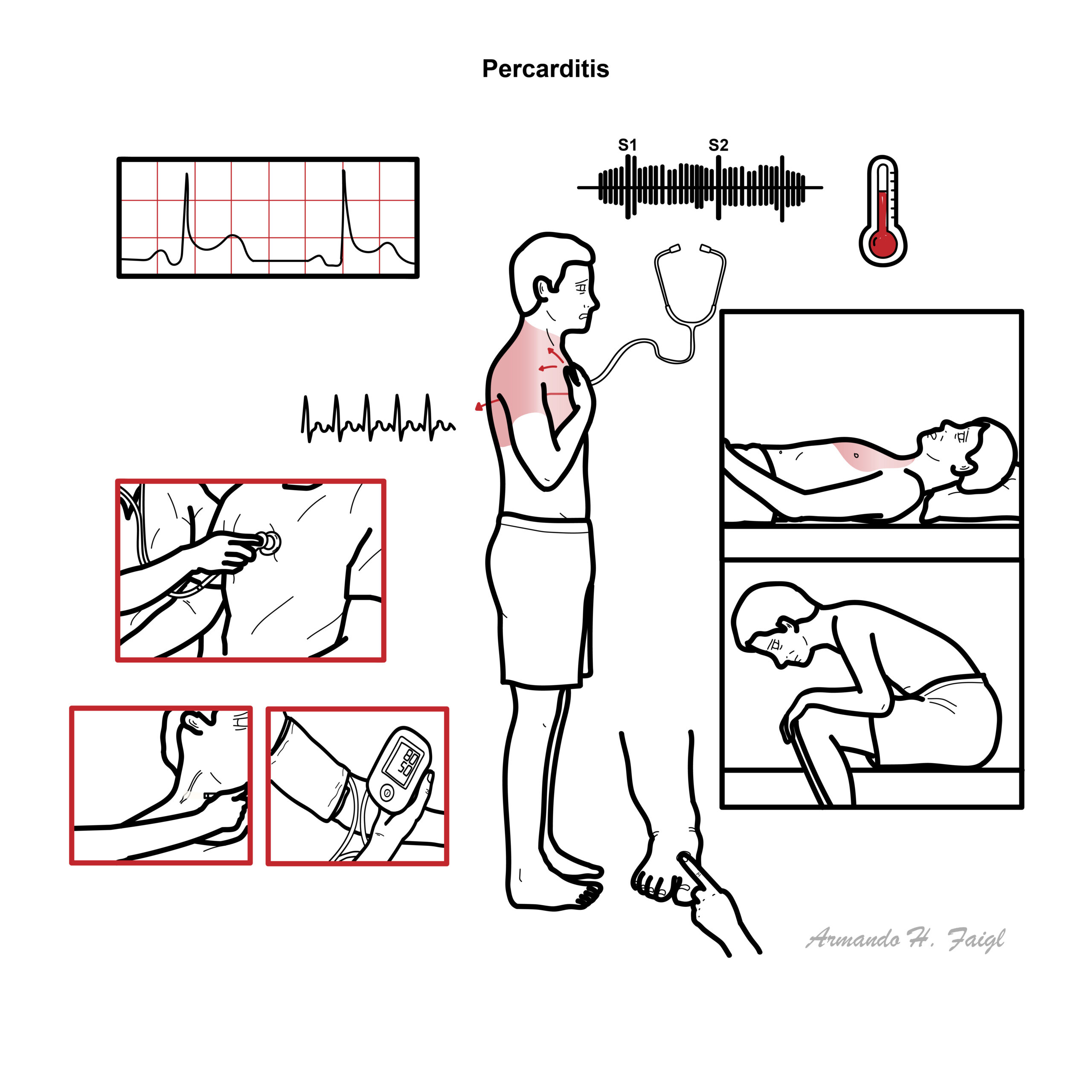
- Fever and malaise
- Sharp retrosternal or left-sided chest pain.
- The pain is often eased by leaning forward and is worse in the supine position
- “pericardial rub” -friction rub on auscultation, often transient –
- Tachycardia
Acute Pericarditis triad: chest pain, friction rub and ECG changes.
Pericarditic pain is typically worse lying flat and improved by leaning forward.
Clinical examination
Pericardial friction rub: superficial scratching sound, best heard at the left lower sternal border with the patient leaning forward.TachycardiaFeverSigns of pericardial effusion:
- Quiet heart sounds
- Raised JVP
Signs of cardiac tamponade:
- Hypotension, Raised JVP, Muffled heart sounds—Beck triad
- Tachycardia
- Pulsus paradoxus
- Shock
Hypotension, raised JVP and an effusion suggest cardiac tamponade, requiring urgent assessment and drainage.
Signs of pericardial constriction:
- Raised JVP
- Peripheral oedema
- Ascites
- Hepatomegaly
- Kussmaul sign
Diagnosis
Remember to differentiate pericarditis from other life-threatening causes of chest pain, including acute coronary syndrome, myocarditis or pulmonary thromboembolism.
- Myocardial Infarction (Acute Coronary Syndrome)
- Pulmonary Embolism
- Pneumonia
- Pneumothorax
- Costochondritis
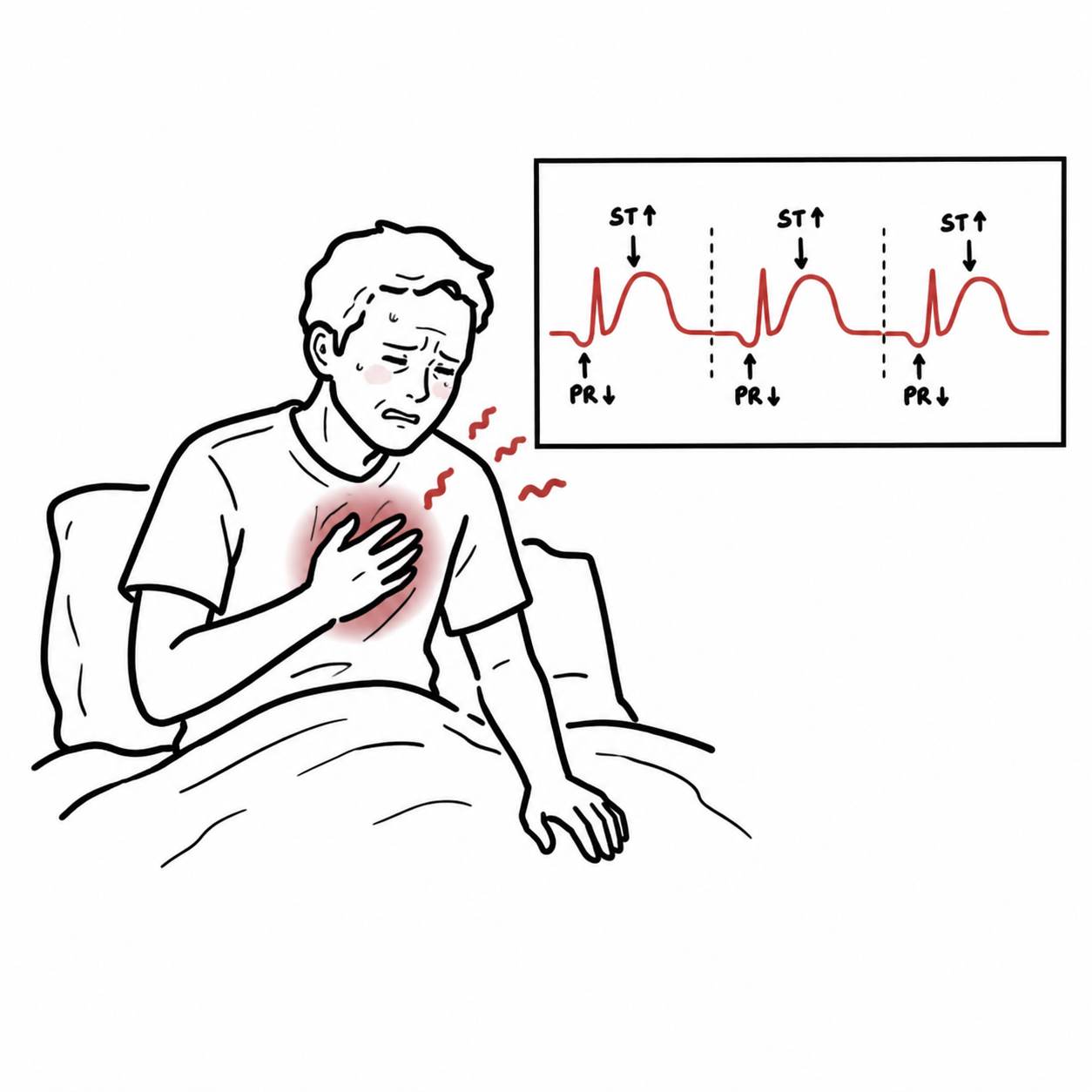
Acute pericarditis is traditionally diagnosed when at least two of four features are present:
- Typical pericarditic chest pain
- Pericardial friction rub
- New widespread ST-segment elevation or PR-segment depression
- New or worsening pericardial effusion
Prompt echocardiography may be required to determine the presence and amount of pericardial fluid.
Other investigations
- ECG
- Troponin: elevated when there is associated myocardial injury.
- CRP and ESR: assess inflammatory activity and help guide treatment duration.
- FBC: leukocytosis, anaemia or evidence of infection.
- UEC and renal function
- LFTs
- Blood cultures if febrile or bacterial infection is suspected.
- Autoimmune or infectious testing only when clinically indicated.
Imaging
- Transthoracic echocardiography: first-line to assess:
- Pericardial effusion
- Cardiac tamponade
- Ventricular function
- Alternative cardiac disease
- Chest X-ray: often normal; cardiomegaly may occur with a large effusion.
- Cardiac MRI: demonstrates pericardial oedema and late gadolinium enhancement and assesses myocardial involvement.
- Cardiac CT: assesses pericardial thickening, calcification and complex anatomy.
| PERICARDITIS VS MYOCARDIAL INFARCTION | ||
| ECG | Acute pericarditis | Acute MI |
| ST-segment elevation | Diffuse in limb leads V2-V6 | Depending on area of infarction (inferior, anterior or lateral) |
| PR-segment depression | Present | Absent |
| QRS complex changes | Absent | Loss of R-wave and development of Q-wave |
Treatment
- NSAIDs + PPIs help relieve symptoms
- Colchicine and steroids are also used for as adjuncts and for more serious cases
- For resistant recurrent pericarditis, seek specialist advice.
Complication management
- Cardiac tamponade: urgent pericardiocentesis or surgical drainage.
- Recurrent large effusion: consider pericardial window or other definitive drainage procedure.
- Constrictive pericarditis: diuretics may temporarily relieve congestion, but definitive treatment for persistent severe disease is pericardiectomy.
NSAID or aspirin plus colchicine is standard first-line treatment for uncomplicated acute pericarditis.
Complications & Prognosis
- Recurrent pericarditis
- Incessant or chronic pericarditis
- Pericardial effusion
- Cardiac tamponade
- Myopericarditis or perimyocarditis
- Ventricular dysfunction and heart failure when myocardial involvement is significant
- Constrictive pericarditis
- Effusive-constrictive pericarditis
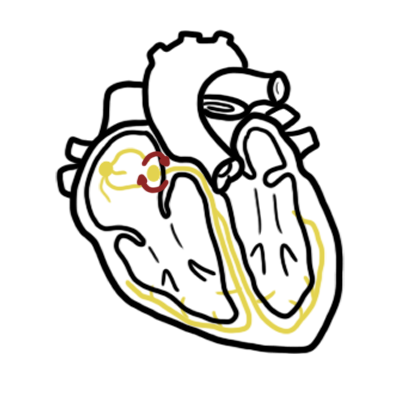
- Arrhythmias
- Rarely, haemodynamic collapse and death.
- Most idiopathic or presumed viral cases have an excellent prognosis and resolve without major complications.
- Recurrence is the most common adverse outcome and is more likely when colchicine is not used or corticosteroids are introduced early or tapered rapidly.
- Cardiac tamponade and constriction are uncommon in idiopathic disease but occur more frequently with bacterial, tuberculous, malignant or purulent pericarditis.
- Prognosis with myopericarditis depends on the degree of myocardial dysfunction.
- Recurrent pericarditis rarely causes death but can produce prolonged pain, disability and impaired quality of life.
Constrictive pericarditis and pericardial effusion can mimic heart failure but both of these can themselves be differentiated.
| Constrictive Pericarditis | Cardiac Tamponade | Heart failure | |
| Kusmaul’s sign | Present | Absent | Absent |
| Pulsus paradoxus | Uncommon | Present | Absent |
| Jugular Venous Pressure (JVP) | Increased | Increased | Increased |
| Percardial Knock (third heart sound, due to rapid ventricular filling’s being abruptly halted by the restricting pericardium) | Present | Absent | Absent |
| Hypotension | Variable | Severe | Variable |
Kusmaul’s sign looks at JVP relationship with breathing. This is different to Kusmaul breathing which is air hunger, rapid deep breathing a sign of metabolic acidosis.
Constrictive pericarditis may show calcifications of the pericardium on chest x-ray or thickened pericardium on echocardiography. Definitive therapy is resection of the pericardium.
References
- Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369(16):1522–1528. doi:10.1056/NEJMoa1208536.
- Schulz-Menger J, Collini V, Groeschel JW, et al. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025.
- Wang TKM, Klein AL, et al. 2025 concise clinical guidance: an ACC expert consensus statement on the diagnosis and management of pericarditis. J Am Coll Cardiol. 2025. doi:10.1016/j.jacc.2025.05.023.
- Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases. Eur Heart J. 2015;36(42):2921–2964. doi:10.1093/eurheartj/ehv318.
- Imazio M, Gaita F, LeWinter M. Evaluation and treatment of pericarditis: a systematic review. JAMA. 2015;314(14):1498–1506. doi:10.1001/jama.2015.12763.




Members only discussions coming soon…