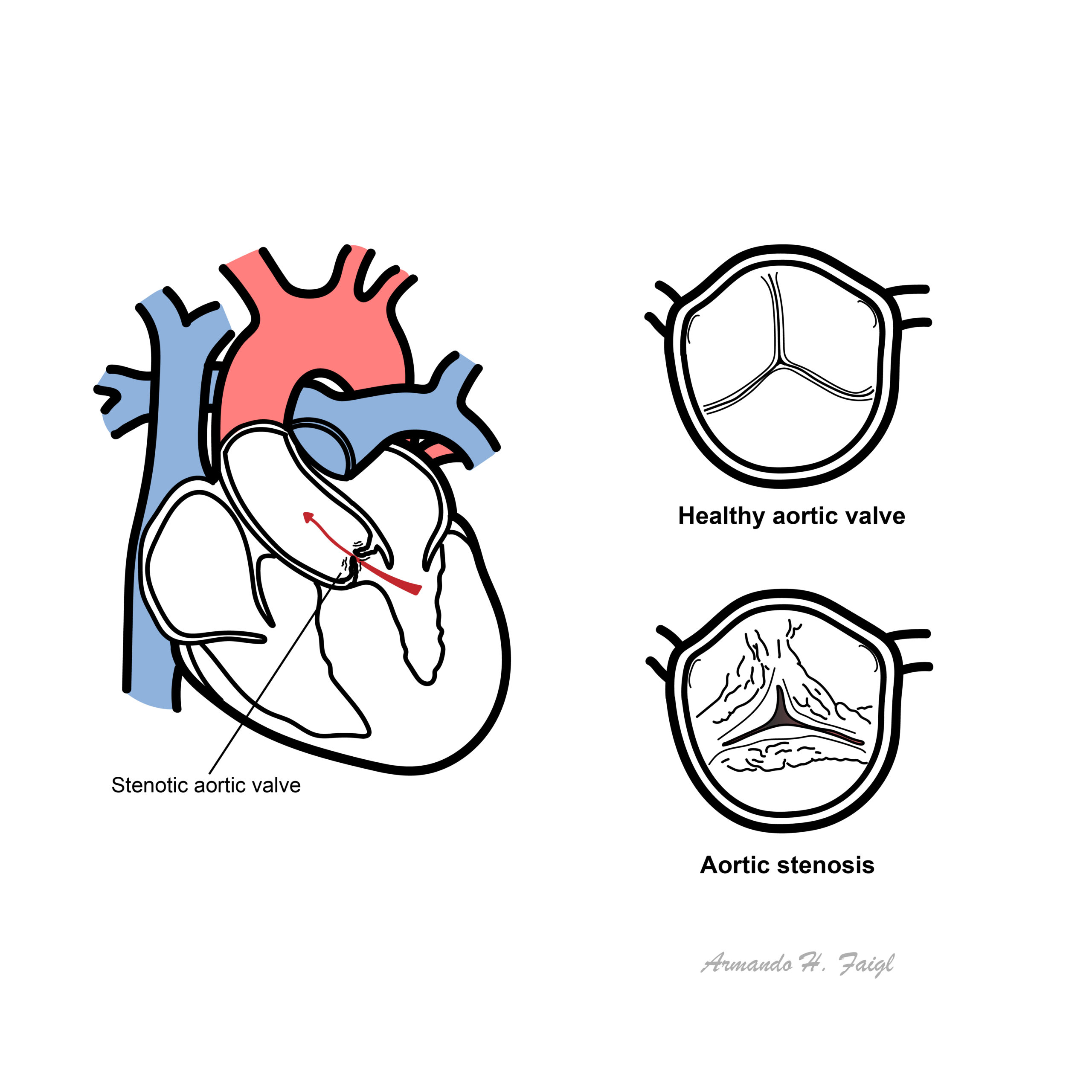
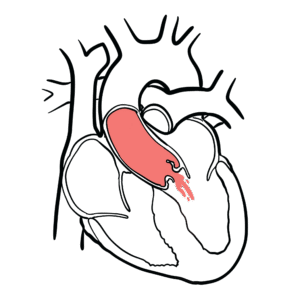
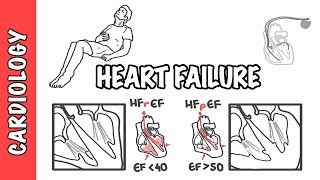
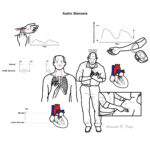
Aortic valve stenosis is characterised by obstruction of left ventricular outflow, resulting in inadequate cardiac output, decreased exercise capacity, heart failure, and death from cardiovascular causes.
Mild to moderate aortic stenosis is usually a symptomatic, but occasionally can be found on routine examination
Locations of stenosis – Valvular (common), supravalvular and subvalvular
Aortic Stenosis produces a “Mid Systolic Murmur”, which is a murmur heard between the first heart sound (S1 – AV valve closure) and ends before the second heart sound (S2 – Aortic and Pulmonary valve closure)
Most common valvular heart disease in western countries and prevalence increase with increasing age
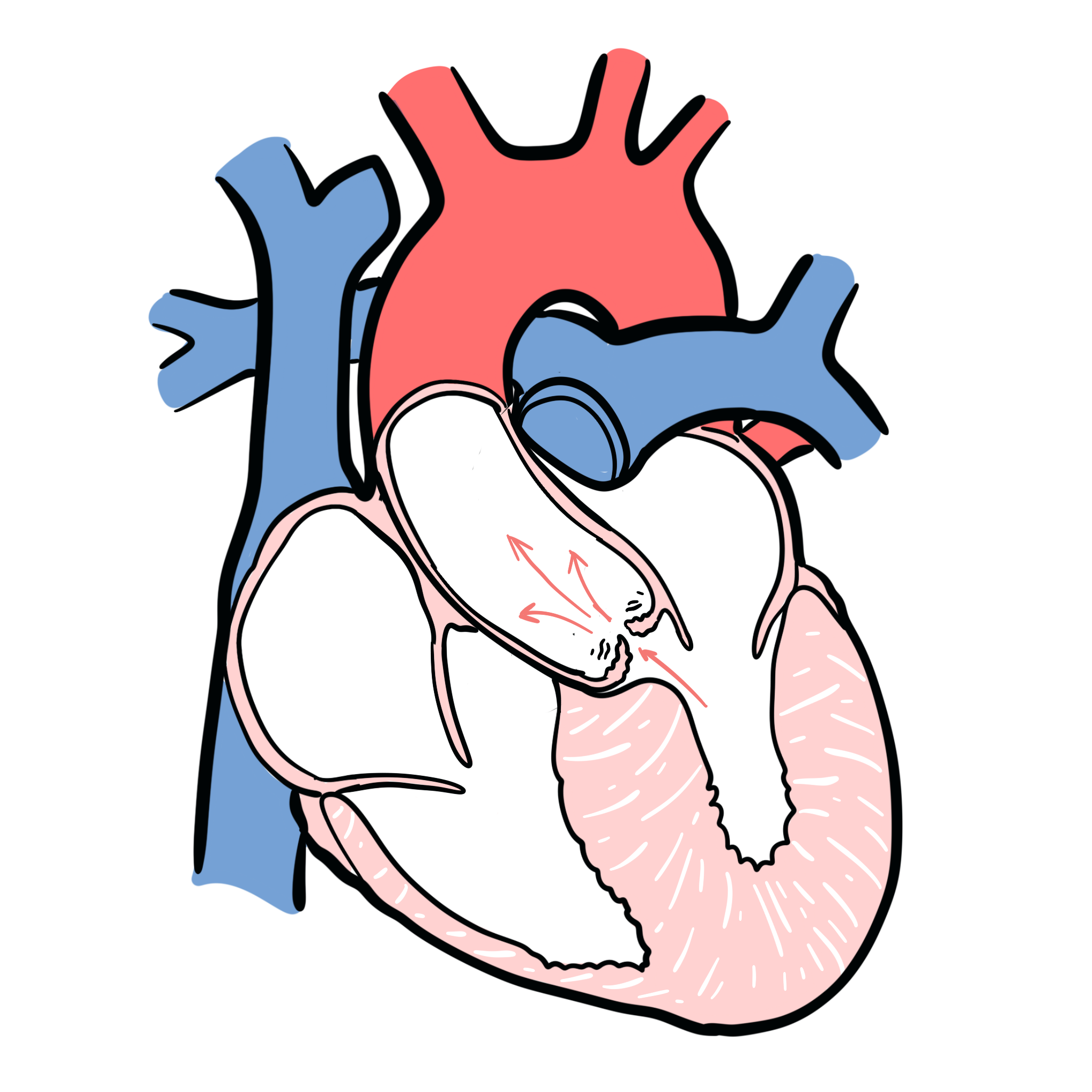
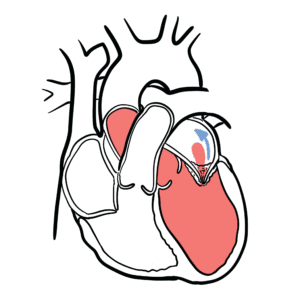
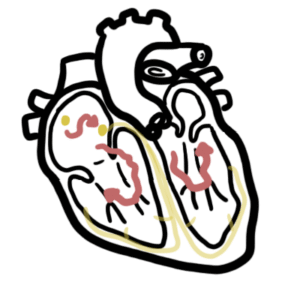
The Mitral and tricuspid valves are atrioventricular valves meaning they allow blood to move from the atrium to the ventricles of the heart. This occurs with ventricular diastole.
The aortic and pulmonary valve are tricuspid valves which when open allow blood to move to the aorta and pulmonary system respectively. This occurs during ventricular systole when the heart contracts.
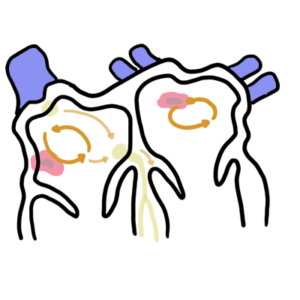
All of the heart valves except the mitral valve are usually tricuspid. However, there can be congenital bicuspid valves which can predispose one to valvular disease later on. The heart valves can be heard most prominent in the following regions of the chest
Aortic valve – Right 2nd intercostal space parasternal
Pulmonary valve – Left 2nd intercostal space parasternal
Tricuspid valve – Left 4th intercostal space parasternal
Mitral valve – Left 5 intercostal space mid-clavicular (below the nipple)
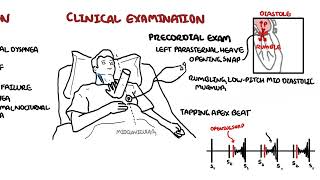
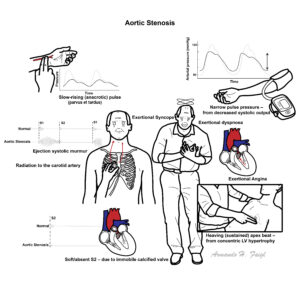
Slow rate of rise in carotid pulse (parvus and tardus)
Auscultation – Aortic Valve (right second intercostal space parasternal)
Ejection systolic murmur – Mid to late peak intensity of the murmur generally begins after S1 and ends before S2 (mid systolic murmur)
Reduced intensity of S2, closing of the aortic valve
Atrial contraction, S4, maybe heard
Auscultation – Apex (Left fifth intercostal space mid-clavicular)
Murmur may radiate to apex of heart
High frequency and louder murmur (Holosystolic murmur) can be confused with mitral regurgitation (Gallavardin phenomenon)
Cardiac Examination findings include parvus and tardus of the carotid artery and mid-systolic ejection murmur heard over the left second intercostal space parasternal. Murmur can radiate to the carotids.
Signs of severity
Parvus et tardus
Aortic thrill
Length, harshness and lateness of the peak of the systolic murmur
Atrial contraction, S4
Parodical splitting of the second heart sound (delayed left ventricular ejection and aortic valve closure)
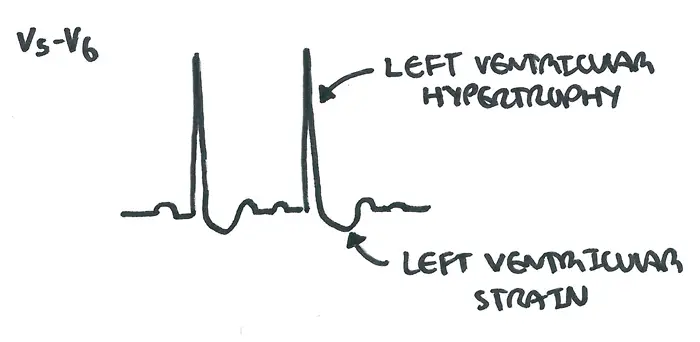
Left ventricular failure
Squatting increases venous return and accentuate the murmur.
This image series is only available to members
Side note – Clinical Auscultation
Murmur
Heart Sound
Mitral Stenosis
High pitched early-diastolic murmur
Loud S1
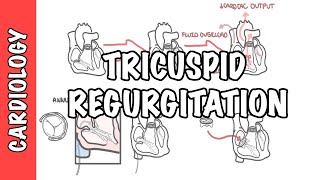
Mitral Regurgitation
Pansystolic murmur radiates to the axilla
Soft S1 loud S2
Aortic stenosis
Ejection systolic “crescendo decresendo” murmur radiating to the carotids
Mortality in patients with AS dramatically increases after the development of cardiac symptoms. The rate of death is 50% at 2 years for patients with symptomatic disease unless aortic valve replacement is performed promptly.
References
Jarcho, JA 2014, “Aortic-Valve Stenosis – From Patients at Risk to Severe Valve Obstruction”, The New England Journal of Medicine, vol. 371, no. 8, pp. 744-56. UpToDate Best Practice











Discussion