

Sexual Transmitted Infection
Overview
Sexually transmitted infections (STI) are a significant public health worldwide. STI can result in chronic disease, pregnancy complications, infertility, and even death. Globally, congenital syphilis is still a leading cause of stillbirth and neonatal death. Antibiotic-resistant Neisseria gonorrhoeae continues to be a significant public health concern. Chlamydia trachomatis infection is the most frequently reported sexually transmitted infectious disease in the United States and continues to be an important risk factor for pelvic inflammatory disease (PID), ectopic pregnancies, urethritis, cervicitis, chronic pelvic pain, and infertility. Treatment of STDs should also include treatment of patients’ partners. Overall, patients, especially the younger population, should be screened regularly and counselled to ensure early diagnosis and treatment. Contraception does not prevent STI, protection such as condoms do.
Definition
STI: Infections that can be spread during sexual contact, some infections like herpes and warts can also be transmitted by skin to skin contact
Contraception: Deliberate use of artificial methods or other techniques to prevent pregnancy as a consequence of sexual intercourse. Methods include barrier methods, contraceptive pill and intrauterine devices. Only the barrier method can prevent STIs
Sex Protection: Safe sex is having sexual contact while protecting yourself and your sexual partner against sexually transmissible infections (STIs) and unplanned pregnancy.
Vaginal swab: First-line investigation for suspicion of STI. You can perform high vaginal swab, low vaginal swab or swab from the cervix itself.
Nucleic acid amplification test: Nucleic acid amplification is a valuable molecular tool not only in basic research but also in application oriented fields, such as clinical medicine development, infectious diseases diagnosis, gene cloning and industrial quality control. Polymerase chain reaction (PCR) was the first nucleic acid amplification method developed and until now has been the method of choice.
PCR: Polymerase chain reaction (PCR) was the first nucleic acid amplification method developed.
Pap smear: Quick and simple test used to check for changes to the cells of the cervix that may lead to cervical cancer.
Premenarche female with signs of STD – sexual abuse?
| Notifiable STI in Australia |
| Chlamydia |
| Donovanosis |
| Gonorrhoea |
| Syphilis |
| Hepatitis |
| HIV |
Clinical Manifestations
- Ulcers, rash, itch around genitals
- Intermenstrual bleeding or post-coital bleeding
- Low abdominal pain
- Dyspareunia
- Dysuria
- Discharge – different, non-physiological
| Characteristic of common cause of vaginal discharge | |||
| Appearence | Smell | Itch | |
| Physiological | Clear/white, mucoid | – | – |
| Foreign body | Grey or bloody, purulent | Offensive | – |
| Malignancy | Bloody, watery | Offensive | – |
| Bacterial Vaginosis | Grey, watery | Offensive | Itchy |
| Trichomonas | Green, frothy | Offensive | – |
| Candidasis | Curd like (cheesy) | – | Itchy |
| Gonococcal | Green, watery | – | – |
Aetiology & Risk Factors
| Risk Factors |
| Unprotected intercourse without male or female condom use |
| Unprotected mouth-to-genital contact |
| Early sexual activity, especially before age 18 |
| Having multiple sex partners |
| Having a high-risk partner (one who has multiple sex partners or other risk factors) |
| Having anal sex or a partner who does |
| Alcohol and Illicit Drug use |
| Exchange of sex (sex work) for drugs or money |
Approach
- History
- Sexual History and partners over the past 12months
- Past STI
- Assess Risk factors
- Examination
- Investigation
- Swab (should be done at presentation)
It is important to note notifiable sexually transmitted infections and also CONTACT TRACING!
Although initial treatment of simple infection may be appropriate without culture, symptomatology can be variable and the gold standard should be a positive culture and sensitivity, especially with persistent or recurrent symptoms.
Pubic lice
Overview
- Pubic lice also known as pthirus pubis is a six-legged insect
- Commonly live in pubic hair areas including armpit.
- Can be transmitted during sexual intercourse or through shared clothes/sheets
Diagnosis
- Identification of the adult lice or their egg (nits) in the affects area
Trichomonas
Overview
- Trichomonas vaginalis
- Flagellated protozoan
- Cervix may have a strawberry appearence (from punctate haemorrhage)
Clinical Presentation
- Asymptomatic (majority)
- Vaginal discharge
- Vulval itching and soreness
- Dysuria
| Characteristic of common cause of vaginal discharge | |||
| Appearence | Smell | Itch | |
| Physiological | Clear/white, mucoid | – | – |
| Foreign body | Grey or bloody, purulent | Offensive | – |
| Malignancy | Bloody, watery | Offensive | – |
| Bacterial Vaginosis | Grey, watery | Offensive | Itchy |
| Trichomonas | Green, frothy | Offensive | – |
| Candidasis | Curd like (cheesy) | – | Itchy |
| Gonococcal | Green, watery | – | – |
Diagnosis
- Vaginal swab → Microscopy on wet smear (normal saline) or acridine orange stained slide
- Culture vaginal swab
- Vaginal Swab/cervical swab → nucleic acid amplification test (gold standard)
Treatment
- Metronidazole
- Partner must be contacted and tested/treated
Pharmacology
Metronidazole is a prodrug. Unionized metronidazole is selective for anaerobic bacteria due to their ability to intracellularly reduce metronidazole to its active form. This reduced metronidazole then covalently binds to DNA, disrupt its helical structure, inhibiting bacterial nucleic acid synthesis and resulting in bacterial cell death. Metronidazole is used against protozoa such as Trichomonas vaginalis, amebiasis, and giardiasis. Metronidazole is extremely effective against anaerobic bacterial infections and is also used to treat Crohn’s disease, antibiotic-associated diarrhea, and rosacea.
Complications
- ↑HIV transmission
In pregnancy Trichomonas infection is associated with preterm delivery and low birth weight baby.
Chlamydia
Overview
- Chlamydia trachomatis
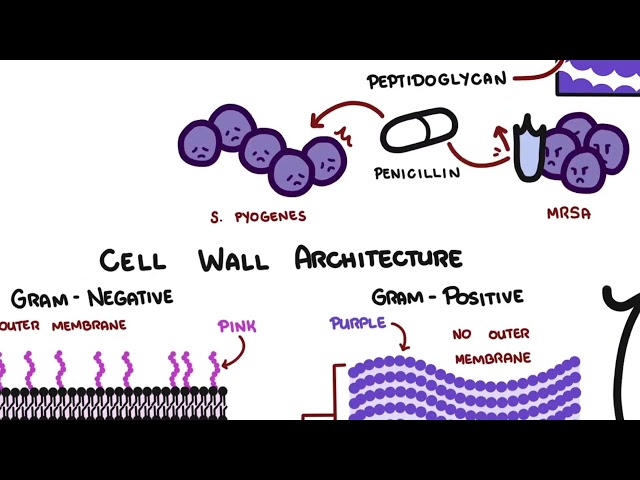
- Gram-negative bacterium that lives as an obligate intracellular parasite
- Most common STI
- Coinfection with neisseria gonorrhoea
Clinical Presentation
- Asymptomatic (70% of cases)
- Dysuria
- Vaginal discharge
- Irregular menstrual bleeding
Diagnosis
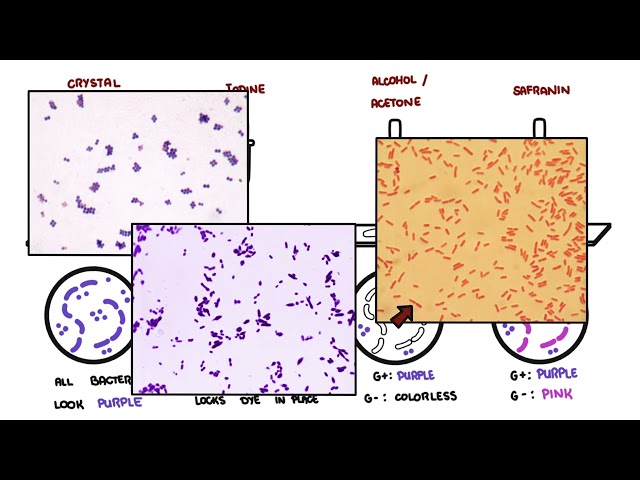
- Vaginal Swab/cervical swab → Gram stain
- Presence of pink “gram -ve”
- Vaginal Swab/cervical swab → Culture
- Vaginal Swab/cervical swab → nucleic acid amplification test (gold standard)
Treatment
- Doxycycline
- Pregnancy use erythromycin (doxycycline is contraindicated)
- Partner must be contacted and tested/treated
In pregnancy chlamydia infection is associated with preterm rupture of membranes. Risks to the baby include neonatal conjunctivites and pneumonia.
Complications
- Pelvic Inflammatory Disease
- Conjuctivitis
- Fitz-Hugh-Curtis syndrome
- Reiter’s syndrome (Reactive Arthritis)
- Tubule infertility
- Risk of ectopic pregnancy
Fitz-Hugh-Curtis syndrome is a rare complication of Pelvic inflammatory disease which involves liver capsule inflammation leading to the creation of adhesions.
Reiter’s syndrome also known as reactive arthritis presents with the classic triad: conjuctivities, urethritis and arthritis. (Can’t see, can’t pee, can’t climb a tree).
Gonorrhoea
Overview
- Neisseria gonorrhoea
- Bacteria – Gram -ve diplococcus
- Second most common STI
- Co-infection with chlamydia trachomatis
Clinical Presentation
- Asymptomatic (majority)
- Vaginal discharge
- Low abdominal pain
- Irregular menstrual bleeding
| Characteristic of common cause of vaginal discharge | |||
| Appearence | Smell | Itch | |
| Physiological | Clear/white, mucoid | – | – |
| Foreign body | Grey or bloody, purulent | Offensive | – |
| Malignancy | Bloody, watery | Offensive | – |
| Bacterial Vaginosis | Grey, watery | Offensive | Itchy |
| Trichomonas | Green, frothy | Offensive | – |
| Candidasis | Curd like (cheesy) | – | Itchy |
| Gonococcal | Green, watery | – | – |
Diagnosis
- Vaginal Swab/cervical swab → Gram Stain
- Presence of pink “gram -ve” diplococcus
- Presence of neutrophils
- Vaginal Swab/cervical swab → Culture
- Check for antibiotic syndrome
- Vaginal Swab/cervical swab → nucleic acid amplification test
Antibiotic-resistant Neisseria gonorrhoeae continues to be a significant public health concern.
Treatment
- Ceftriaxone + azithromycin
- Pregnancy same treatment
In Pregnancy the risk of gonorrhoea infection to the baby is opthalmia neonatarum (50% of cases).
Complications
- Pelvic Inflammatory Disease (10% of cases)
- Bartholin’s or Skene’s abscess
- Migratory polyarthralgia
- Septic arthritis
- Tubule infertility
- Risk of ectopic pregnancy
Bartholin’s abscess (cyst) The bartholin glands are located bilaterally at the base of the labia minora. Obstruction of the distal Bartholin’s duct may result in the retention of secretions, with resultant dilation of the duct and formation of a cyst. The cyst may become infected, and an abscess may develop in the gland. A Bartholin’s duct cyst does not necessarily have to be present before a gland abscess develops.
Syphilis
Overview
- Treponema pallidum
- Bacteria – spiral looking (spirochete)
Clinical Presentation Syphilis can present in one of latent different stages
- Primary
- Occurs 1week-3 months post infection
- Painless genital ulcers (chancre)
- Inguinal lymphadenopathy
- Secondary
- Occurs within 2 years of infection
- Fever
- Polymorphic rash affecting palms, soles and everywhere else
- Genital chondyloma lata
- Lymphadenopathy
- Anterior uveitits
- Latent
- no signs and sympoms before tertiary syphilis
- Tertiary (not contagious)
- Occurs after 2 years of infection, but may take >40yrs to develop
- Neurosyphilis
- Cardiovascular syphilis
- Gunmata (inflammatory plaques or nodules)
| STDS with Ulcers |
| Chancroid (Painful) |
| Syphilis (Painless |
| Herpes (Painful) |
Diagnosis
- Treponemal enzyme immunoassay
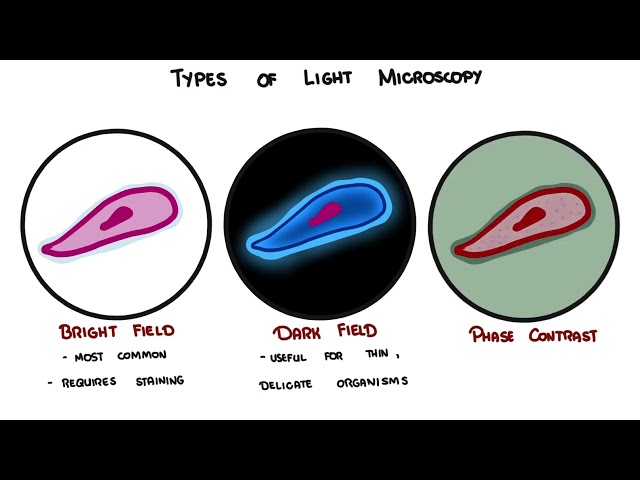
- Primary syphilis ulcer smear may show spirochaetes on dark feild microscopy
Treatment
- Benzylpenicillin (1st line)
- Erythromycin – If allergic to penicillin
- Doxycycline – If allergic to penicillin (contraindicated in pregnancy)
Complications
In Pregnancy syphilis infection can result in preterm delivery, stillbirth, congenital syphilis and miscarriage.
Bacterial Vaginosis
Overview
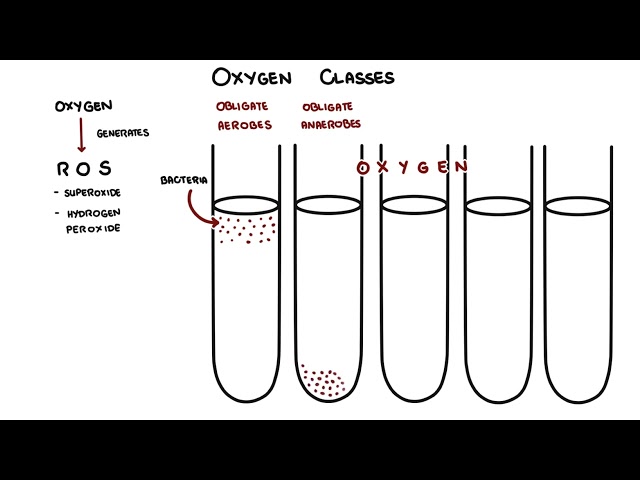
- Mixed anaerobes: Gardnerella and Mycoplasma hominis which replace the usually dominant vaginal lactobacilli
- Common cause of abnormal vaginal discharge in young women
- NOT SEXUALLY TRANSMITTED
- 12% of women will experience bacterial vaginosis at some point in their lives
Clinical Presentation
- Asymptomatic (majority)
- Smelly vaginal discharge “fishy”
| Characteristic of common cause of vaginal discharge | |||
| Appearence | Smell | Itch | |
| Physiological | Clear/white, mucoid | – | – |
| Foreign body | Grey or bloody, purulent | Offensive | – |
| Malignancy | Bloody, watery | Offensive | – |
| Bacterial Vaginosis | Grey, watery | Offensive | Itchy |
| Trichomonas | Green, frothy | Offensive | – |
| Candidasis | Curd like (cheesy) | – | Itchy |
| Gonococcal | Green, watery | – | – |
Diagnosis – Amsel criteria 3 out of 4 required
| Amsel criteria |
| Homogenous whitish grey discharge |
| Vaginal pH >4.5 (5.5?) |
| Fishy smell of vaginal discharge |
| Presence of ‘clue cells’ on microscopy |
Treatment
- Metronidazole
- Avoid vaginal douching/overwashing which can destroy natural vaginal flora
Complications
- ↑Pelvic infection post surgery
In pregnancy bacterial vaginosis is associated with mid-trimester miscarriage, preterm rupture of membranes and preterm delivery.
Candidiasis
Overview
- Candidiasis is a fungal infection caused by yeasts that belong to the genus Candida
- Candidiasis that develops in the mouth or throat is called “thrush” or oropharyngeal candidiasis
- Candida albicans (90% )
- Risk factors: immunosupressoin, antibiotics, pregnancy, diabetes mellitus and anaemia
- Nearly 75% of all adult women have had at least one “yeast infection” in their lifetim
Clinical Presentation
- Asymptomatic
- Vulval itch or soreness
- Thick, cur-like vaginal discharge
- Dysuria
- Classic white plaques on vaginal wall
| Characteristic of common cause of vaginal discharge | |||
| Appearence | Smell | Itch | |
| Physiological | Clear/white, mucoid | – | – |
| Foreign body | Grey or bloody, purulent | Offensive | – |
| Malignancy | Bloody, watery | Offensive | – |
| Bacterial Vaginosis | Grey, watery | Offensive | Itchy |
| Trichomonas | Green, frothy | Offensive | – |
| Candidasis | Curd like (cheesy) | – | Itchy |
| Gonococcal | Green, watery | – | – |
Diagnosis
- Characteristic appearance
- Vulval and vaginal aerythema
- Vulval fissuring
- White plaques on vaginal wall
- Microscopic – wet slide show spores and pseudohyphae
Treatment
- Only treat if asymptomatic
- Azoles +/- topical azoles
Pharmacology
Azole inhibit fungal inhibitis enzymes responsible for the synthesis of ergosterol. Ergosterol is an essential component of the fungal cell membrane, inhibition of its synthesis results in increased cellular permeability causing leakage of cellular contents. Side effects: symptoms of overdose include hallucinations and paranoid behavior.
Complications
- Not significant
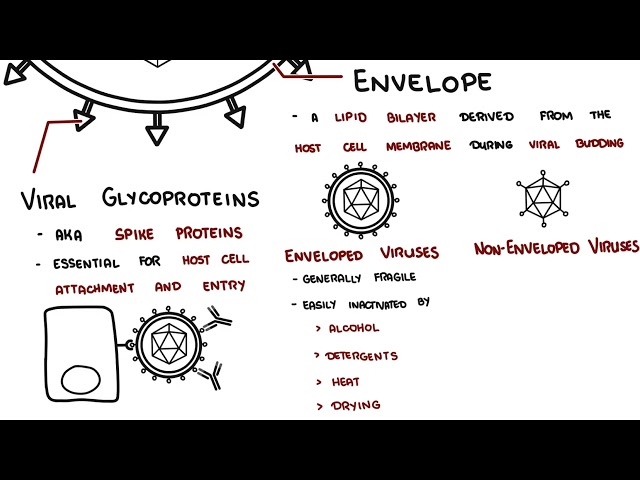
Herpes Simplex
Overview
- Herpes Simplex Virus type 1 and type 2
- HSV-1 cause oral and genital ulcers
- HSV-2 cause genital ulcers only
- Both HSV-1 and HSV-2 are chronic and lifelong infections
- HSV-1 is mainly transmitted by oral-to-oral contact to cause oral herpes (which can include symptoms known as “cold sores”), but can also cause genital herpes.
- Symptoms of herpes include painful blisters or ulcers at the site of infection.
- Herpes infections are most contagious when symptoms are present but can still be transmitted to others in the absence of symptoms.
Clinical Presentation
- Similar for HSV-1 and HSV-2 infections.
- Patients will often experience prodromal symptoms
- Tingling
- Itching
- Paresthesias
- Pain from an hour to a day before the outbreak
- Flu-like symptoms +/- inguinal lymphadenopathy
- Ulcers develop – lesions typically heal within 5 to 10 days.
- Patients with HSV-1 infections typically have fewer outbreaks than patients with HSV-2 infections.
Diagnosis
- Presence of classic herpes rash
- PCR testing of vesicular fluid
- Culture of vesicular fluid
Treatment
- Not cure for gential herpes
- Symptomatic relief – analgesia, topical anaesthetic
- Oral aciclovir
- Topical aciclovir
- Condoms or abstinence whilst prodromal or sympatomatic → ↓transmission
Pharmacology
Aciclovir is an antiviral drug that acts as an antimetabolite, inhibits DNA synthesis by acting as a chain terminator. Aciclovir is used for the treatment of herpes simplex virus infections, varicella zoster (chickenpox) and herpes zoster (shingles). Side effects: Nephrotoxicity and neurotoxicity, which usually resolve after cessation of aciclovir therapy.
Complications
- Meningitis
- Encephalitis
- Keratitis
- Sacral radiculopathy
- Transverse melitis
- Depression – with stigma
In pregnancy herpes infection can lead to neonatal herpes a rare, but sometimes fatal, condition that can occur when an infant is exposed to HSV in the genital tract during delivery.
Human Papillomavirus
Overview
- HPV is the most common sexually transmitted infection
- Many types of HPV
- Responsible for cervical cancer and genital warts
- HPV types 6 and 11 cause 90% of genital warts (Condyloma accuminatum)
- HPV types 16 and 18 cause 70% of cervical cancers
Clinical Presentation – condyloma accuminatum
- Asymptomatic (majority)
- Painless genital lumps
- Perianal warts (no association with anal intercourse)
Diagnosis
- Clinical appearence
- Pap smear
Treatment for genital warts
- Clinic Treatment – Ablation
- Cryotherapy
- Trichloroacetic acid
- Laser
- Home treatment (contraindicated in Pregnancy)
- Podophyllotoxin cream
- Imiquimod cream
Complications
- HPV types 6 and 11 cause 90% of genital warts
- HPV types 16 and 18 associated with high-grade CIN and cause 70% of cervical cancers
References
Drugbank.ca
CDC
Oxford Handbook of Obstetrics and Gyaenacology









Members only discussions coming soon…