

Bronchiectasis
Overview
Bronchiectasis was a common disabling and fatal condition in the pre-antibiotic era and remains more common in medically underserved regions of the world.
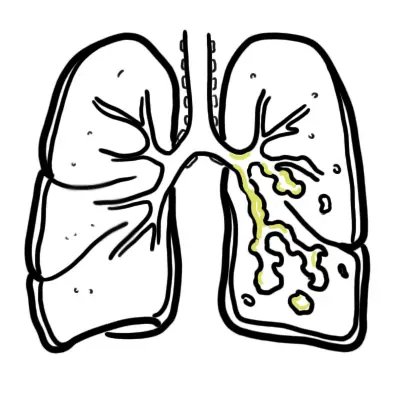
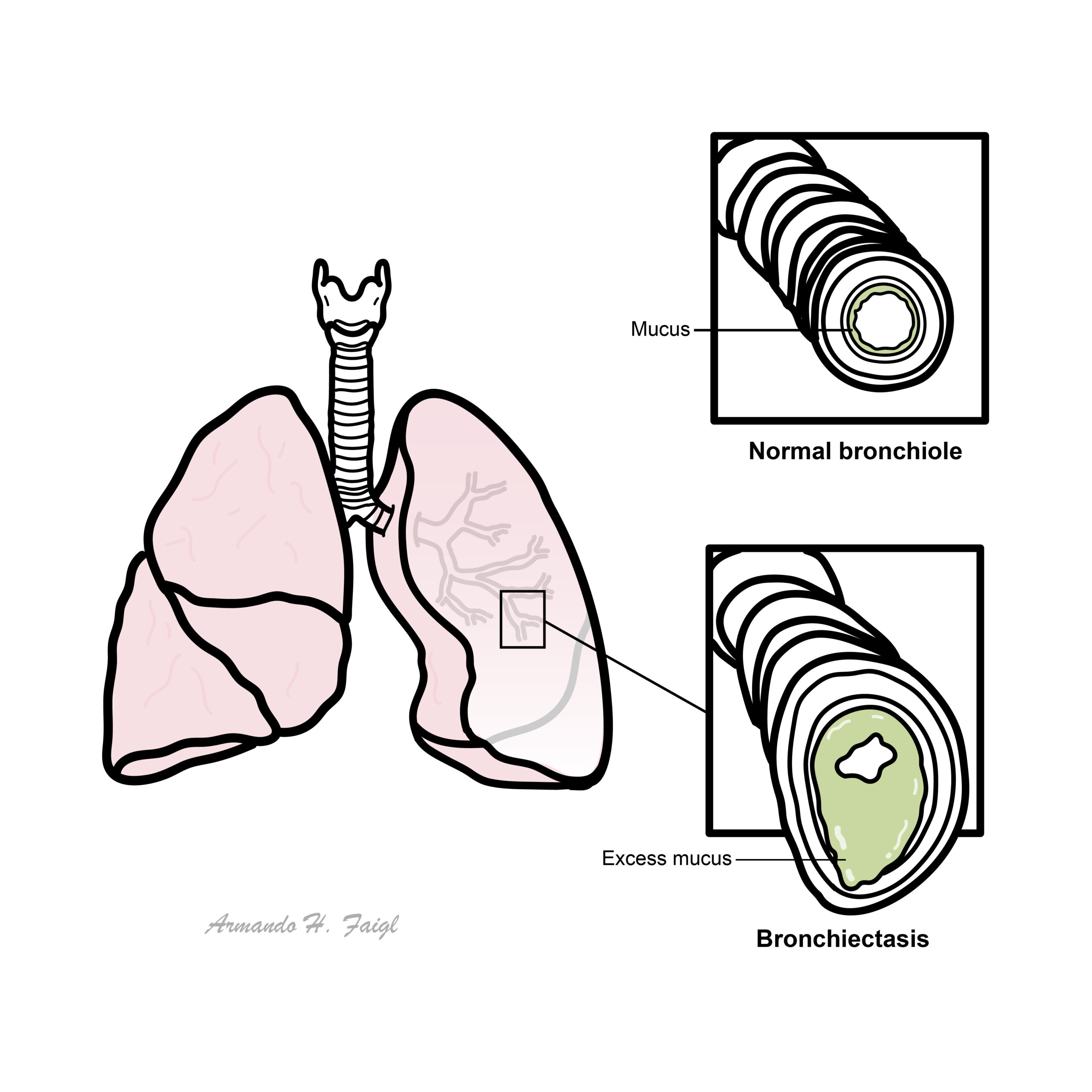
Irreversible dilatation of airways due to in ammatory destruction of airway walls resulting from persistently infected mucus. Bronchiectasis usually affects medium sized airways
Definition
Bronchiectasis: Bronchiectasis is the permanent dilation of bronchi due to the destruction of the elastic and muscular components of the bronchial wall.
Cystic Fibrosis (CF): The major cause of chronic debilitating pulmonary disease and pancreatic exocrine deficiency in the first three decades of life. It is characterized by the triad of chronic obstructive pulmonary disease, pancreatic exocrine deficiency, and abnormally high sweat electrolyte concentrations. Characteristic pancreatic changes give the disease its name.
Clubbing: Increase in the angle between the nail and nail base of 180° or greater, and softening of the nail base to palpation. Although the condition can be familial, clubbing is uncommon in children, usually indicating chronic pulmonary, hepatic, cardiac, or gastrointestinal disease.
Aetiology & Risk Factors
Aetiology
The most common cause of bronchiectasis is post infection. Connective tissue disease, cystic fibrosis are other common causes.
It almost always involves the respiratory tract; most patients develop bronchiectasis by the age of 18 months, although some may not experience respiratory difficulty for several years.
- Cystic fibrosis
- Host immunodeficiency
- Previous infections
- Congenital disorders of the bronchial airways
- Primary ciliary dyskinesia
- Alpha-1 antitrypisn deficiency
- Connective tissue disease
- Inflammatory bowel disease
- Aspiration or inhalation
Pathophysiology
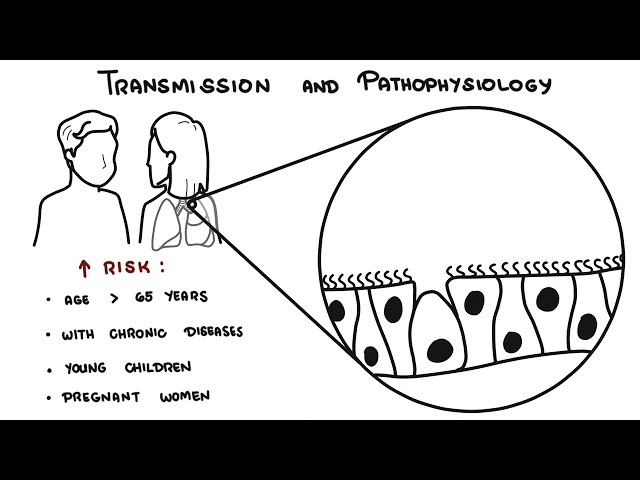
Essentially the different causes of bronchiectasis with impaired respiratory defences/ immunodeficiency will trigger an inflammatory process, recurrent infections that will result in the pathological changes seen bronchiectasis. There will be bronchiole dilatation, immune cells infiltration into the tissue (lymphocytes), bronchial ulceration and oedema, smoother muscle hypertrophy and neovascularization.
Patients with bronchiectasis gets recurrent infection. Common causes of infections are p. aureginosa, s. pneumoniae, h. influenzae, s. aureus. Infection can trigger exacerbations.
oral corticosteroids for acute, major exacerbations.
Clinical Manifestation
Clinical Presentation
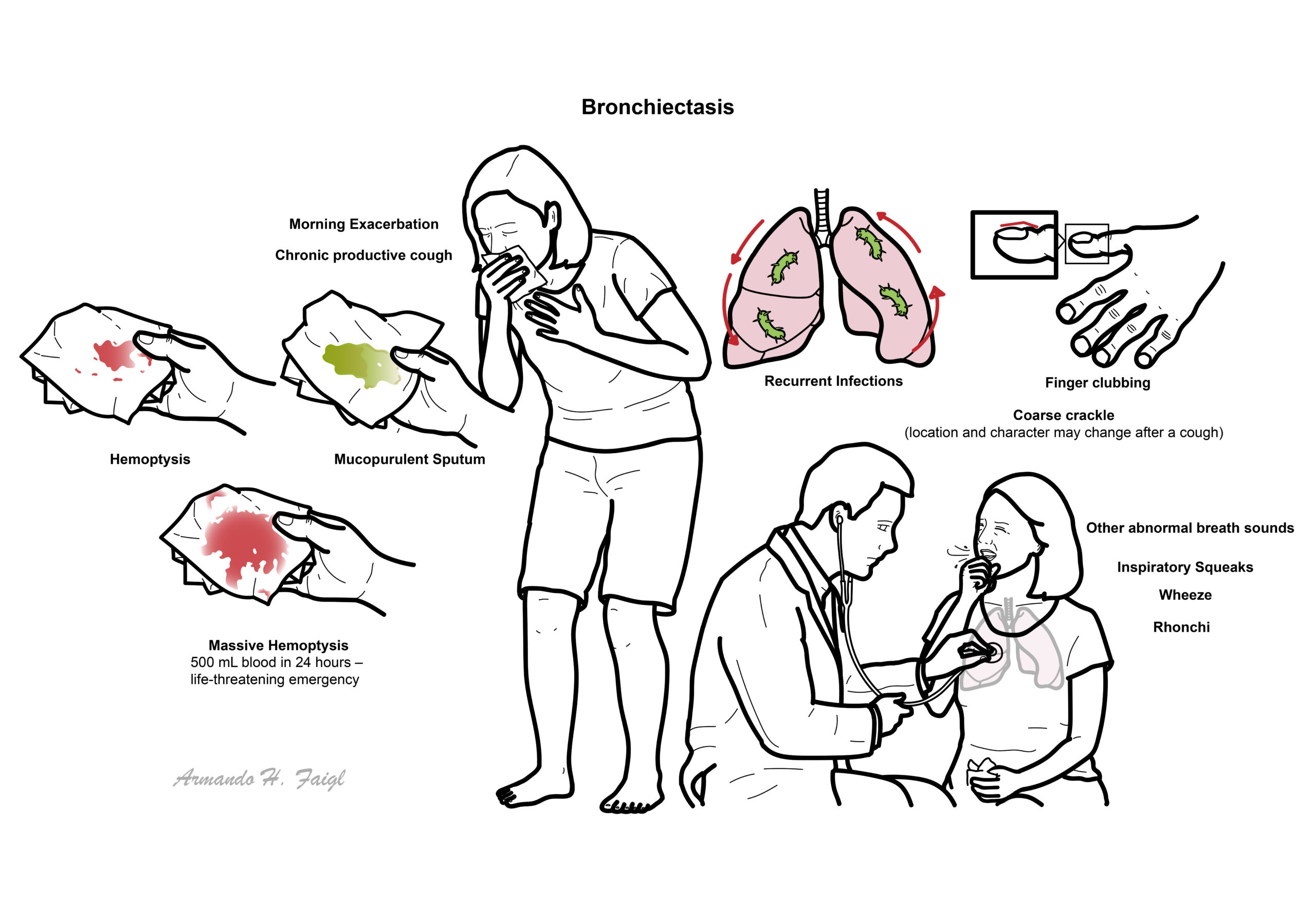
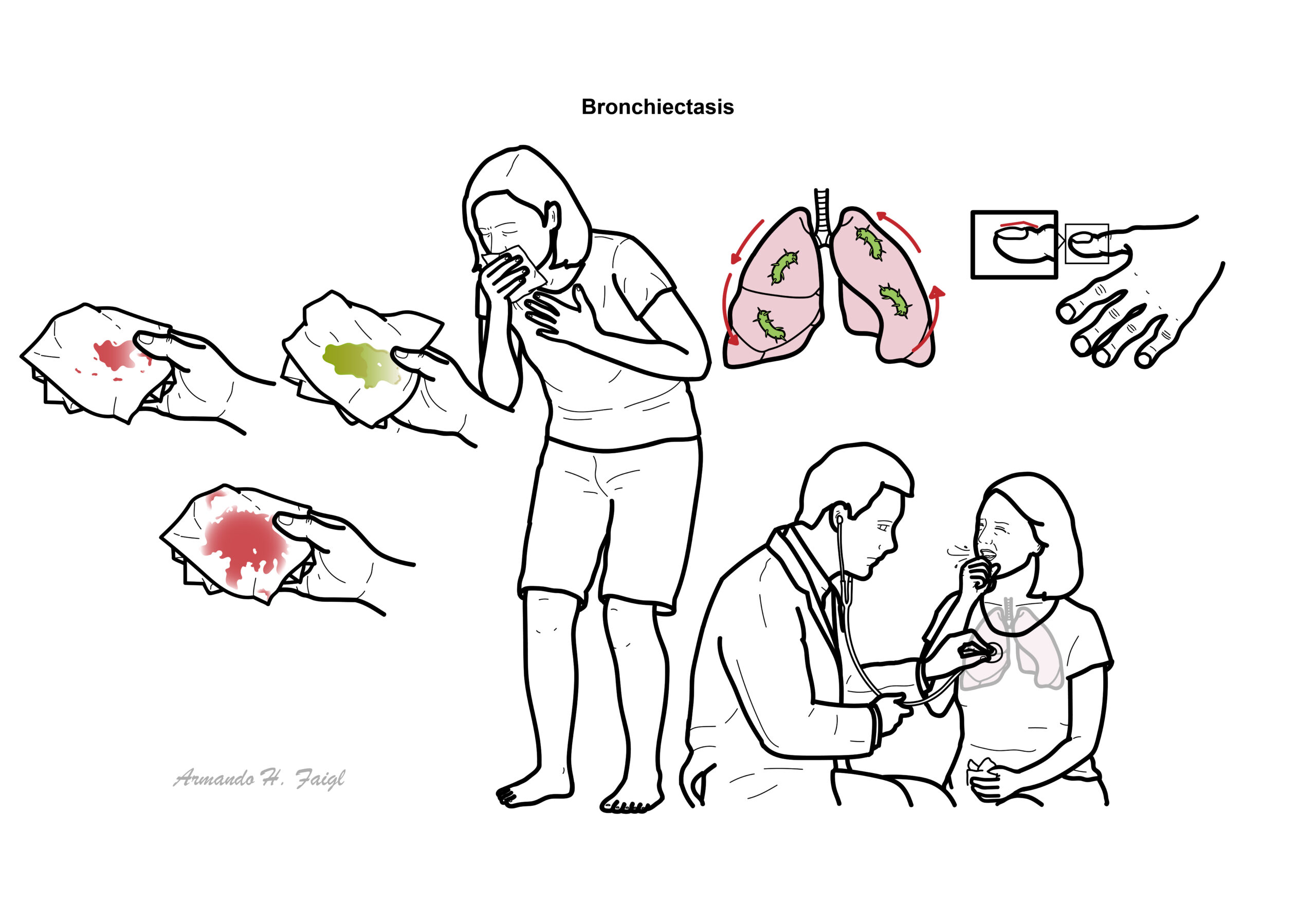
The classic clinical manifestations of bronchiectasis are daily cough and mucopurulent sputum production. Cough is invariably present and often may be the only symptom for years. Purulent, tenacious sputum production, frequently worse in the morning (having accumulated during recumbency in sleep) is present in most patients. Presentation is usually with the background of a recent viral infection, connective tissue disease or cystic fibrosis. Can present with haemoptysis.
Massive haemoptysis is >500ml blood loss in 24hrs.
Examinations
Percussion resonant, mixed predominant coarse crackles, often additional polyphonic wheeze. Presence of of high pitch inspiratory squeals and rhonchi.
Diagnosis
Bronchiectasis is a type of COPD. Other types of COPD include emphysema, chronic bronchitis and asthma.
FBC and immunloglobulin studies are important in CT is now the defining test for the diagnosis of bronchiectasis. Chest x-ray show the presence of increased pulmonary markings, ring-like structures, atelectasis, dilated and thickened airways (tram lines), and mucus plugging (finger-in-glove) appearance; however, the chest radiograph may be normal even in the presence of bronchiectasis.
Treatment
Vaccination, chest physiotherapy. Inhaled/oral/IV antibiotic used for mild-severe exacerbations. Inhaled corticosteroids is standard to decrease inflammation. Oral steroids for exacerbations. Finally pulmonary resection in selected cases with focal bronchiectasis.
to treat the underlying cause as well (ie. cystic fibrosis, Rheumatoid arthritis, Inflammatory bowel disease).
Complications & Prognosis
- Massive haemoptysis
- Respiratory failure
- Cor pulmonale
- Bronchiectasis is an irreversible condition.
- The typical disease course consists of periods of symptom control interrupted by periods of exacerbations.
- Bronchiectasis frequently co-exists with other respiratory disease, making it difficult to determine prognosis for bronchiectasis alone.
References
- UpToDate
- Bestpractice
- Toronto notes 2016
- Case Files Internal Medicine 4th ed.






Members only discussions coming soon…