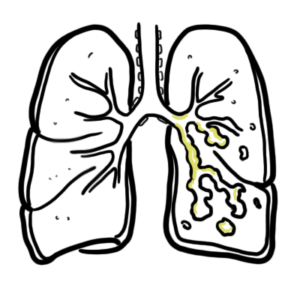
0:00 Bronchectasis is defined by the presence of permanent dilation –ectasia of 0:12 the bronchi. 0:15 In bronchectasis there is also excessive mucous production resulting in reduced 0:21 airflow. 0:22 Interestingly, severe infections such as pneumonia and tuberculosis were the 0:27 predominant causes 0:28 of bronchiectasis. 0:31 After the introduction of antibiotics, the thought was that the incidence would 0:35 decrease. 0:36 Sadly, this is not the case, and the number of patients with bronchiectasis has 0:40 risen, 0:40 placing an increasing burden on global healthcare systems. 0:45 Recurrent infections cause bronchiectasis, but nearly all diseases affecting 0:50 the lung 0:51 can lead to bronchiectasis through different mechanisms. 0:55 The main clinical significance of bronchiectasis is once it's established, it 1:02 leads to recurrent 1:04 airway infections by bacteria and fungi organisms. 1:09 And then this will obviously cause the chronic cough, sputum production, weight 1:16 loss, and 1:16 respiratory compromise. 1:21 The respiratory tract is important in delivering oxygen from the upper 1:28 respiratory tract to 1:29 the lower respiratory tract, which is made up of the trachea, the bronchi, the 1:35 bronchioles, 1:36 and finally to the alveoli for gas exchange, where oxygen is exchanged for 1:43 carbon dioxide. 1:45 The bronchi are lined by epithelial cells. 1:49 Let's take a look at the normal defense or protective mechanisms of the 1:53 respiratory 1:54 tract. 1:56 So the epithelium represents a physical barrier built to resist infections 2:02 through tight cellular 2:04 junctions. 2:05 Mucus is produced by goblet cells here to trap bacteria and foreign stuff. 2:10 The epithelium have the mucosillary apparatus, which sweeps and transports bad 2:15 things up the 2:16 respiratory tract into the esophagus, the stomach to be digested. 2:22 There are antimicrobial peptides produced such as lysosymes, secretory leuk 2:27 ocyte protease 2:28 inhibitors, defense sins, and whatnot to help protect the area from microbes. 2:34 There's a cough reflex, which helps clear things from the lungs, either out of 2:38 the body 2:39 or into the stomach, so that can be destroyed. 2:43 You also have antibodies, IgA antibodies, which help target pathogens for 2:48 clearance by the 2:49 innate immune cells such as the neutrophils and the macrophages. 2:54 All these mechanisms are thought to contribute and are impaired in bronchiect 2:59 ases, because 3:00 it increases bacterial colonization in the lungs and susceptibility to 3:06 infections, the 3:07 primary pathological hallmark in bronchiectases. 3:12 So it has been postulated that there are two distinct phases of disease in bron 3:19 chiectases. 3:21 The first is the insult to the airway epithelium. 3:27 And this initial insult causes the initial bronchial dilatation and the mucos 3:34 illary impairment. 3:36 This initial phase predisposes one to infection and inflammation. 3:44 First insult will lead to the second phase, which is the ongoing inflammatory 3:49 cycle and 3:50 further infections. 3:54 And because of this, you finally get permanent airway remodeling. 4:00 The characteristic of bronchiectases, which is dilatation of the airways, with 4:05 excessive 4:05 mucus production. 4:08 So this first insult to the airway epithelium we talked about can be from many 4:15 causes. 4:16 So some examples include cystic fibrosis. 4:21 Cystic fibrosis is a well-known cause of bronchiectasis. 4:24 It is an autosomal recessive disease caused by mutation in the cystic fibrosis 4:30 transmembrane 4:30 conductance-regulated gene, or CFTR gene. 4:35 So the CFTR gene codes for essentially chloride channels, which helps 4:40 facilitate chloride 4:41 ions out into the airway lumen. 4:45 CFTR gene mutation results in thick mucus, because water is reabsorbed together 4:51 with 4:51 sodium. 4:53 This thick mucus causes an impaired mucosillary apparatus, increasing the risk 4:58 of pulmonary 4:59 infections, and persistent inflammation. 5:04 Another cause of bronchiectasis is airway obstruction, which can be caused by a 5:10 foreign 5:10 body being aspirated, an interluminal obstructing lesion, such as a carcinor 5:16 tuma, or an extra 5:18 luminal cause compressing the airway, such as from lymph node. 5:26 Calcium results in local inflammatory response, causing damage to the endothel 5:31 ium, and subsequently 5:32 mucosillary apparatus dysfunction, increasing the risk of infection and 5:39 inflammation. 5:40 Other causes include tracheobronco-malacia, or tracheobronco-megli. 5:46 These are essentially anatomical defects of the airways. 5:51 Another cause of bronchiectasis can be any cause of a defective host defense. 5:56 So, impairment in host defenses may be local, such as in ciliary dyskinesia, or 6:02 primary 6:03 ciliary dyskinesia. 6:05 On a side note, an example of this could be Cartagena syndrome, which is a high 6:12 yield thing 6:12 to know, which is essentially someone with bronchiectasis, or this primary c 6:17 iliary dyskinesia, 6:19 and sinus inverteous. 6:27 Defective host defenses can be systemic, such as someone who has hypogama glob 6:31 inemia, 6:33 so this means low immunoglobulins, low antibodies, increasing the risk of 6:37 infections. 6:38 Defective host defense can be a result of prolonged immunosuppression, such as 6:42 a transpine patient. 6:43 The mechanism of bronchiectasis in patients with defective host defense is 6:47 likely from 6:48 bronchial wall injury, from repeated infections. 6:54 Psych and other systemic diseases, such as Schrogens or SLE, can be complicated 6:59 by bronchiectasis 7:01 through the development of interstitial lung disease, the use of immunosupp 7:06 ressive agents, 7:08 or other unknown mechanisms. 7:15 Another cause of bronchiectasis is alpha-1 anti-tripsin deficiency. 7:19 So, emphysema is the main lung disease recognized in alpha-1 anti-tripsin 7:24 deficiency, but also 7:25 bronchiectasis. 7:27 Alpha-1 anti-tripsin is a protease inhibitor. 7:31 It protects the lower airways from damaged cause by proteolytic enzymes, such 7:36 as elastase. 7:37 So as you can imagine, if someone is deficient in alpha-1 anti-tripsin, this 7:41 means that you 7:42 get more inflammation in the lung. 7:45 Then other causes of bronchiectasis include COPD and asthma. 7:50 Pulmonary infections, so a spectrum of bacterial, myobacterial, atypical 7:55 bacteria, and viral 7:56 lung infections have been associated with the development of bronchiectasis. 8:07 There's something called ABPA, which is allergic bronchol pulmonary aspergill 8:12 osis, which represents 8:13 a hyperimmune reaction to the aspergillus organism, rather than a true 8:18 infection. 8:19 And it's characterized by an exaggerated T helper cell response. 8:28 Features of ABPA include blood e-synophilia, very high plasma IgE levels, and 8:35 precipitating 8:35 and specific antibodies to aspergillus. 8:43 More rare causes of bronchiectasis include polycystic kidney disease, ataxia 8:49 telangic 8:50 tasia, as well as mafan syndrome. 8:56 So all these conditions will lead to bronchiectasis and will predispose one to 9:02 developing recurrent 9:03 pulmonary infections and inflammation, a vicious cycle. 9:08 Infection of the lungs triggers inflammation to surrounding lung epithelia. 9:12 The damaged epithelial cells triggers an inflammatory response. 9:17 The injured epithelial and tissue macrophages will begin secreting pro- 9:22 inflammatory cytokines, 9:24 including interleukin-8, which will recruit more neutrophils, the kamikaze 9:29 cells. 9:29 You also have interleukin-1B and TNF alpha, secreted by the macrophages and 9:34 also surrounding 9:35 cells, which will recruit more immune cells, including monocytes. 9:40 And these will cause mucous gland to hypertrophy, as well as cause hypersec 9:48 retion of mucus. 9:50 And as we know, hypersecretion of mucus, productive cough is a hallmark of bron 9:55 chiectasis. 9:56 The activated neutrophils will release various proteolytic enzymes, such as el 10:01 astase and 10:02 metalloproteinases. 10:04 And this causes surrounding damage to the tissues, causing airway damage, 10:08 damaging celery apparatus, 10:10 and causing mucus hypersecretion. 10:13 The damaged airways again create a vulnerable environment for reinfection. 10:21 Very neutrophilia is the hallmark of bronchiectasis, although up to one-quarter 10:25 , one-third of 10:26 patients have isinophil dominant airway inflammation. 10:31 And this may reflect the different triggers of bronchiectasis. 10:36 So an infection will favor neutrophils and allergies and the environment, 10:40 factors will 10:41 favor isinophilia being present. 10:47 The damaged bronchi increases susceptibility to chronic colonisation by certain 10:52 microorganisms 10:53 such as pseudomonas ariginosa, non-tuberculous myobacterium, as well as asperg 11:00 illus. 11:00 The bacteria most frequently isolated from airway secretions of patients with 11:05 bronchiectasis 11:06 include hemophilus, influenza, and pseudomonas ariginosa. 11:18 So multiple factors may cause reduced celery beating, so disruption in the muc 11:20 osillary apparatus 11:23 as mentioned. 11:25 And again, this can include cyanide produced by the pseudomonas ariginosa, as 11:29 well as the 11:30 neutrophils proteases. 11:35 The clinical features of bronchiectasis are a cough. 11:41 And the daily production of nucoprolant and tenacious sputum, lasting months to 11:48 years, 11:48 less specific complaints include dyspnea, wheezing, and pleuritic chest pain. 11:57 Chemoptysis can be present from injured vessels secondary to inflammation. 12:03 Remember, bronchiectasis should be suspected in patients with chronic cough, 12:08 producing 12:09 large amounts of sputum. 12:12 So investigations for bronchiectasis, now the diagnosis of bronchiectasis can 12:17 be made from 12:18 history of recurrent respiratory infections and also radiological findings. 12:25 On chest x-ray, findings can include acystic shadow, thickened bronchial walls, 12:32 called 12:32 tram lines, however, gold standard of diagnosing bronchiectasis is high- 12:38 resolution CT chest 12:39 scan. 12:40 So here you can see acystic-type pattern of bronchiectasis. 12:44 At any point in the lung, the internal luminal diameter of the bronchus should 12:51 be smaller 12:52 than the external diameter of the adjacent blood vessel. 12:56 The diagnostic radiological criteria for bronchiectasis is therefore when the 13:01 airway diameter 13:03 is greater than that of its accompanying vessel and lack of distal airway tap 13:10 ering. 13:11 A bronchial arterial ratio of greater than one is pathological. 13:18 Some say you need a high-res CT chest findings plus airway neutrophilia to 13:24 diagnose bronchiectasis. 13:26 Further, on the CT chest, bronchiectasis can be categorized into three types 13:34 based on its 13:34 morphology. 13:36 You have cylindrical bronchiectasis, and you can note the dilatation of the 13:40 bronchi. 13:41 You have varicoid bronchiectasis, which is like varicose veins in the legs, and 13:46 then 13:47 you have sacula or cystic bronchiectasis, which is very big dilation, dilat 13:51 ation of 13:52 the bronchi. 13:54 Other investigations include spirometry, which often shows an obstructive 13:58 pattern. 13:59 Bronchoscopy to locate site of hemoptasis and exclude obstruction and obtain 14:04 samples 14:05 for culture. 14:06 You can also perform serum immunoglobulins to look for, obviously, one of the 14:11 causes, 14:12 a hypo gamma globinemia. 14:15 In addition to airway inflammation, there is evidence of systemic inflammation 14:19 associated 14:20 with increased levels of fibrinogen, a coagulation factor, which has been 14:25 proposed as an indirect 14:26 marker of disease severity. 14:29 One can also perform the cystic fibrosis sweat test if they suspect cystic fib 14:33 rosis 14:33 as a cause. 14:35 Also other investigations include aspergillus precipitins, as well as a skin 14:43 prick test. 14:45 Treatment for bronchiectasis, in general. 14:47 So firstly, recommending one to stop smoking and have yearly vaccination is 14:54 recommended. 14:54 Home oxygen may be required if they meet the criteria. 14:58 There's also postural drainage, which should be performed twice daily, and this 15:02 is where 15:03 one goes to specific posture so that they can drain all this mucal, pterol, and 15:07 stuff 15:08 out of their body. 15:09 Chest physiotherapy may age sputum output and mucous drainage. 15:14 Other useful things include breathing techniques, as well as pulmonary 15:18 rehabilitation for adult 15:20 patients as it improves exercise tolerance and health-related quality of life. 15:26 Antibiotics may also be used in the management of chronic bronchiectasis to 15:29 eradicate organisms 15:31 such as pseudomonas arreginosa. 15:34 If someone with bronchiectasis has three or more exacerbations a year, one can 15:40 consider 15:40 long-term antibiotics, and macrolides are the class of oral antibiotics of 15:47 choice, because 15:48 they have both anti-inflammatory and immunomodulatory properties. 15:53 So this includes azithromycin, essentially its first line. 15:59 Inhaled bronchodilators such as nebulae subbeautable may be useful in patients 16:04 with asthma, COPD, 16:05 and ABPA, inhaled steroids are not recommended. 16:12 Surgical resection of bronchiectatic lungs or lobectomy is indicated in certain 16:17 situations. 16:17 For example, if one has bleeding in the lungs, so pulmonary hemorrhage, or the 16:22 bronchus is 16:23 just not viable, it's just damaged. 16:27 So this is a general treatment of people who have bronchiectasis, but then you 16:31 have treatment 16:32 if someone has an exacerbation of their bronchiectasis, and really if someone 16:37 has exacerbation 16:38 of their bronchiectasis, the treatment is guided by sputum cultures and sensit 16:45 ivities. 16:47 Empirical antibiotic therapy is recommended and may be based on previous 16:51 culture data 16:52 until the result of the current sputum cultures become available. 16:57 If there's no previous sputum data or anything available, then a fluoroquinol 17:04 one, such as 17:05 siprofloxacin, can be started to ensure pseudomonas coverage until sputum 17:10 culture results are 17:11 available. 17:12 And I guess one thing to remember is that one of the side effects of siproflox 17:15 acin is 17:16 Achilles tendon rupture. 17:19 There's a large variation in prognosis. 17:25 So with some patients having mild bronchiectasis for many years, and others 17:32 progressing rapidly 17:32 with frequent exacerbations and accelerated lung function decline. 17:45 Now I want to end this video by talking about two diseases that are associated 17:48 with bronchiectasis, 17:49 so it can be a potential cause I guess. 17:53 The first is yellow nail syndrome. 17:56 It's a rare disorder characterized by the triad of yellow thicken nails, lymp 18:02 hedema, and 18:03 respiratory manifestations, typically cough, usually bronchiectasis, or plural 18:10 fusions. 18:11 This is seen at about 50% of people, this triad. 18:14 Treatment includes vitamin E, treating the bronchiectasis, and use of antifung 18:17 als for the 18:18 nails.