

Achilles Tendinopathy & Rupture
Overview
Achilles tendinopathy & rupture are common causes of posterior ankle pain and disability, particularly in active adults. Tendinopathy presents with chronic pain, stiffness, and impaired function, while rupture is an acute injury characterised by a sudden “pop” and loss of plantarflexion power. Achilles tendon injuries are increasingly prevalent due to sports participation, with rupture incidence ~18/100,000 annually, most often in men aged 30–50 years.

Definition
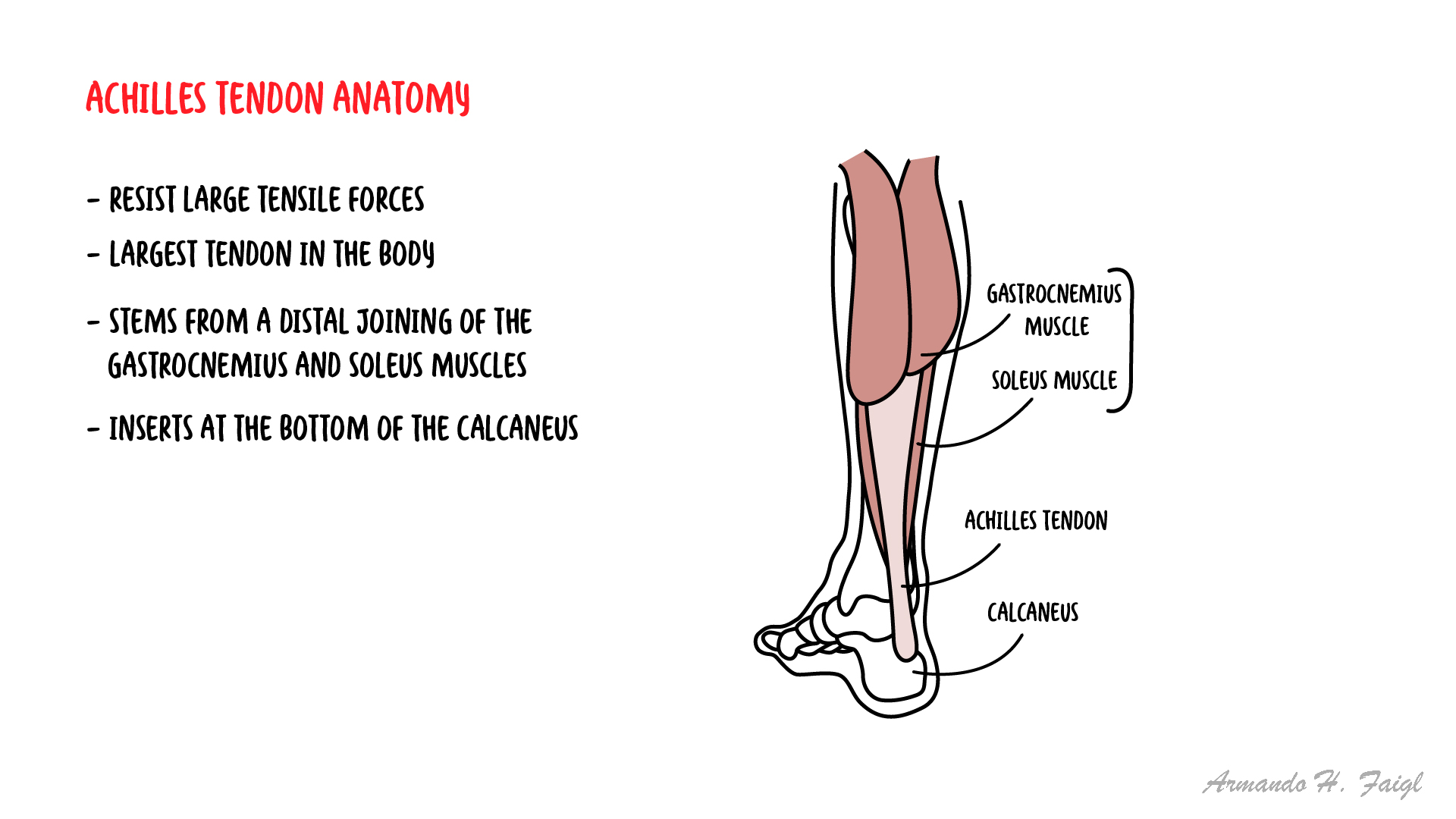
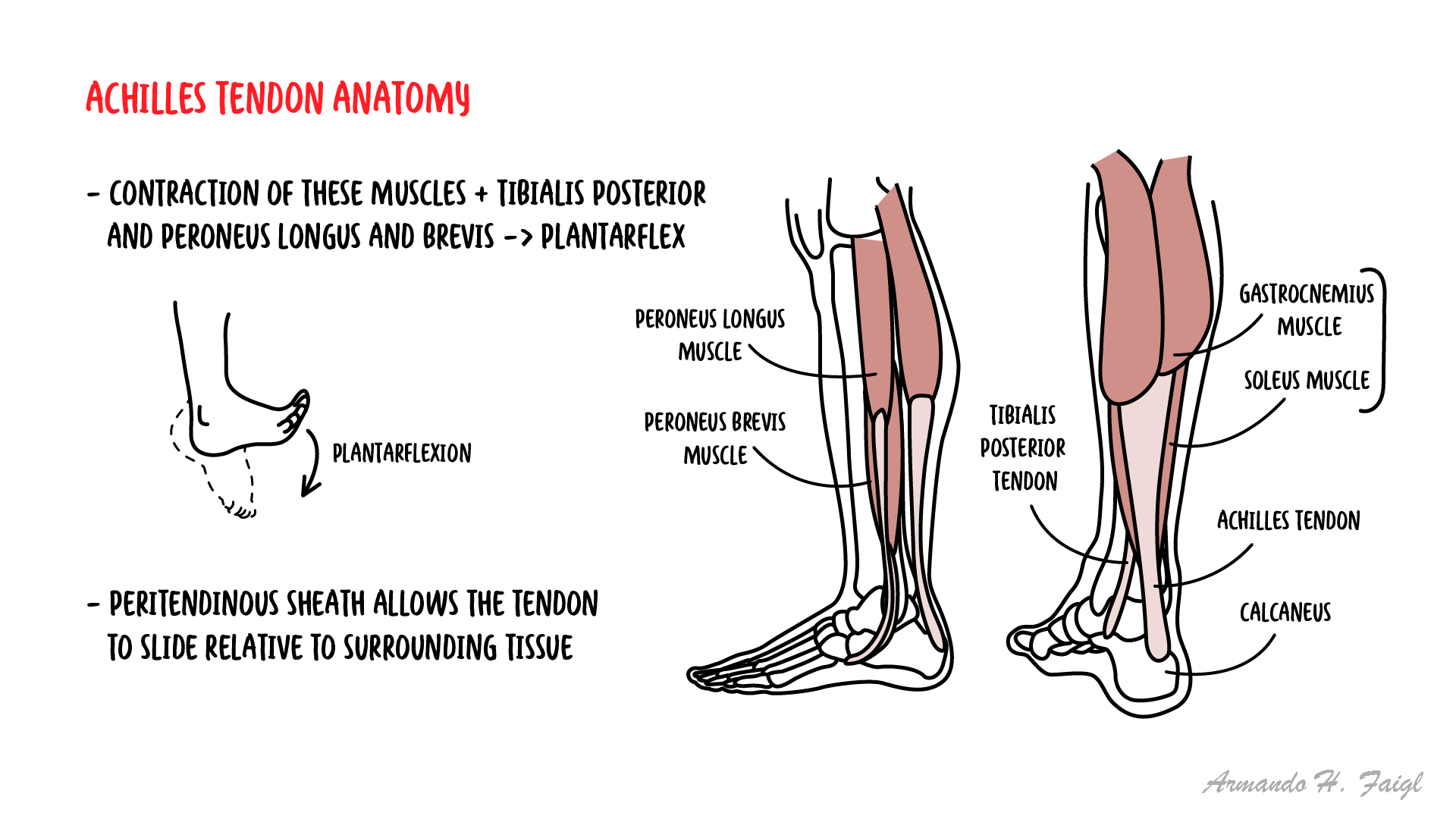
Achilles tendon: Convergence of gastrocnemius and soleus tendons inserting into calcaneus; strongest tendon in the body.
Tendinopathy: Chronic degenerative process of tendon collagen, not just inflammation.
Rupture: Complete disruption of tendon fibres.
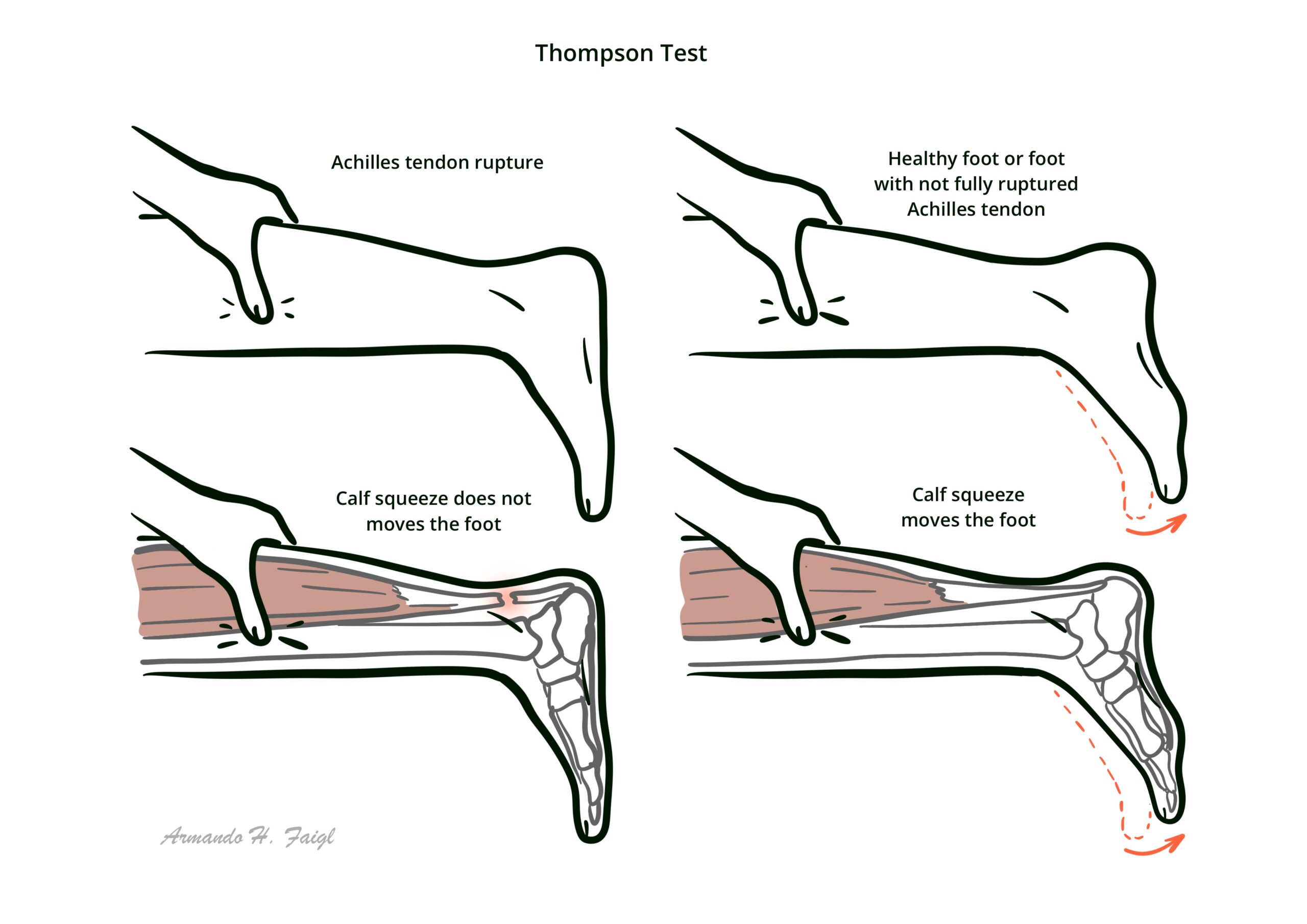
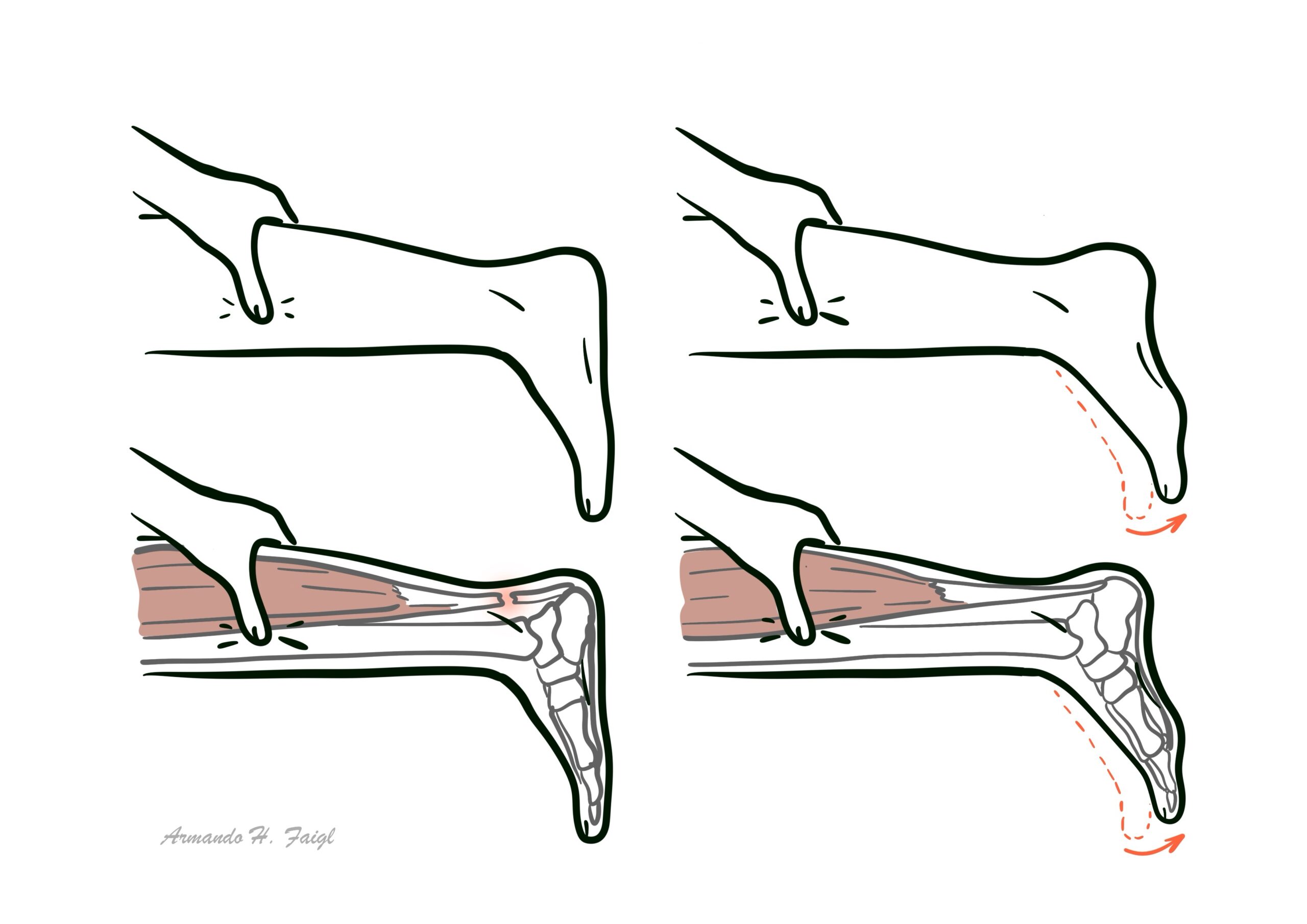
Thompson test: Calf squeeze test; absence of plantarflexion = Achilles rupture.
Anatomy & Physiology
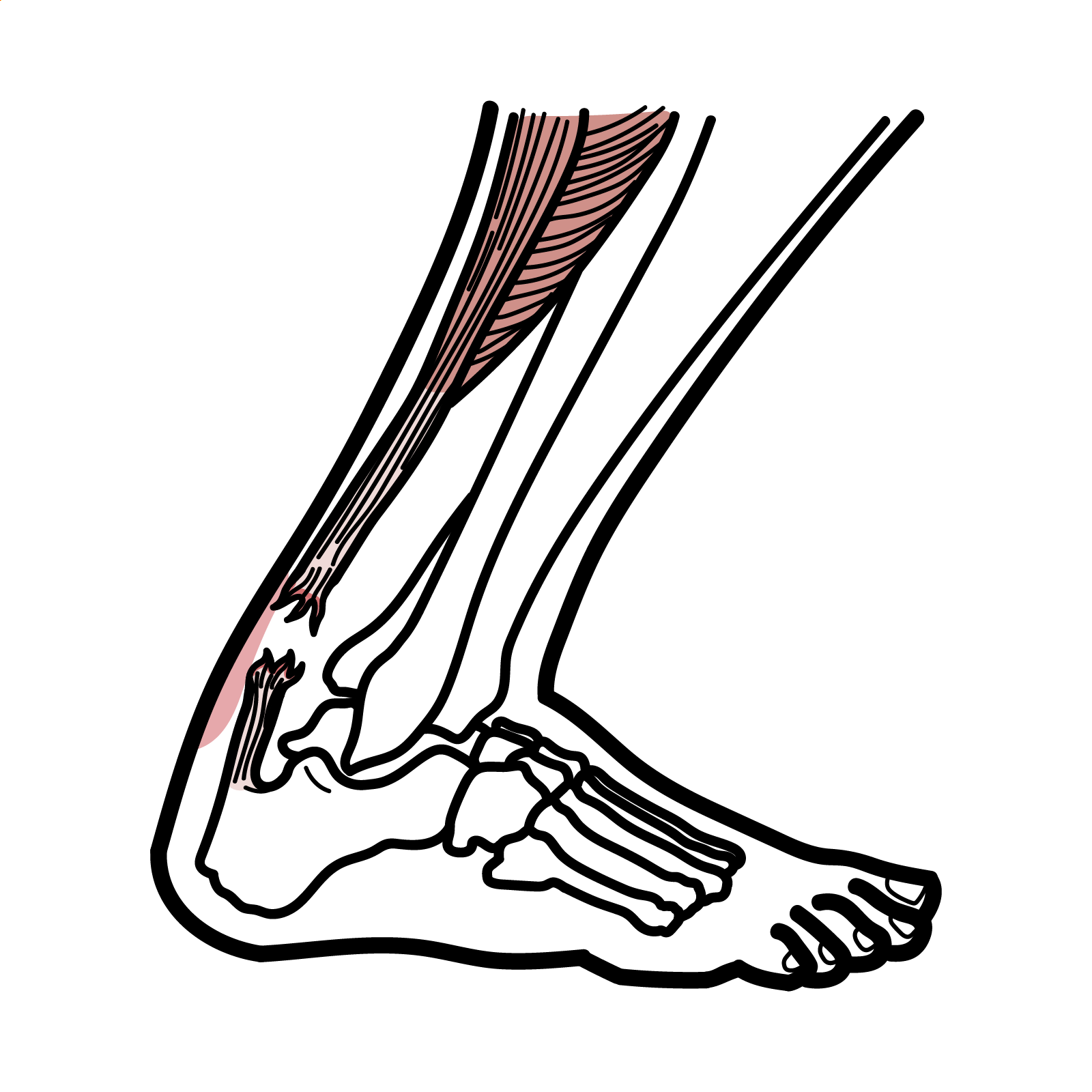
- Structure: Achilles tendon inserts into posterior calcaneus; critical for plantarflexion.
- Blood supply: Relatively hypovascular, especially 2–6 cm proximal to calcaneal insertion → common rupture site.
- Function: Transmits gastrocnemius–soleus force → push-off in gait and jumping.
Ruptures usually occur in the hypovascular “watershed zone.”
Aetiology and Risk Factors
Aetiology
- Tendinopathy
- Chronic overload, repetitive microtrauma.
- Degenerative changes in tendon matrix.
- Rupture
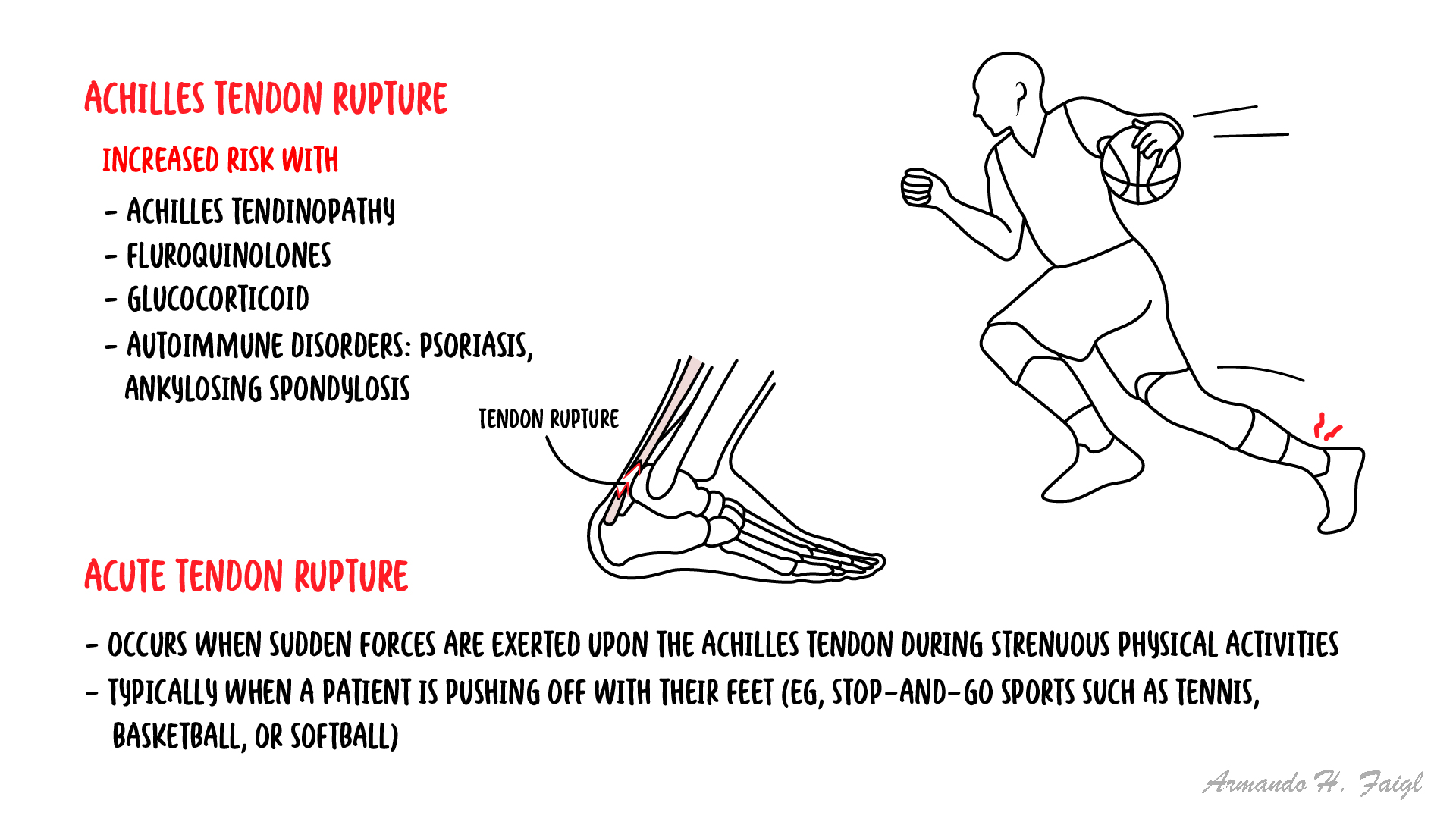
- Sudden eccentric loading (e.g., sprinting, jumping).
- Often occurs in previously asymptomatic tendon.
- Middle-aged “weekend warriors.”
- Quinolone or corticosteroid use (including Cushing’s Disease)
- Prior tendinopathy or rupture.
- High BMI, poor conditioning.
- Systemic diseases (RA, gout, diabetes).
There are other causes of achilles tendon rupture other than sports. These include Quinolones (such as ciprofloxacin) and prolonged corticosteroid use.
Pathophysiology
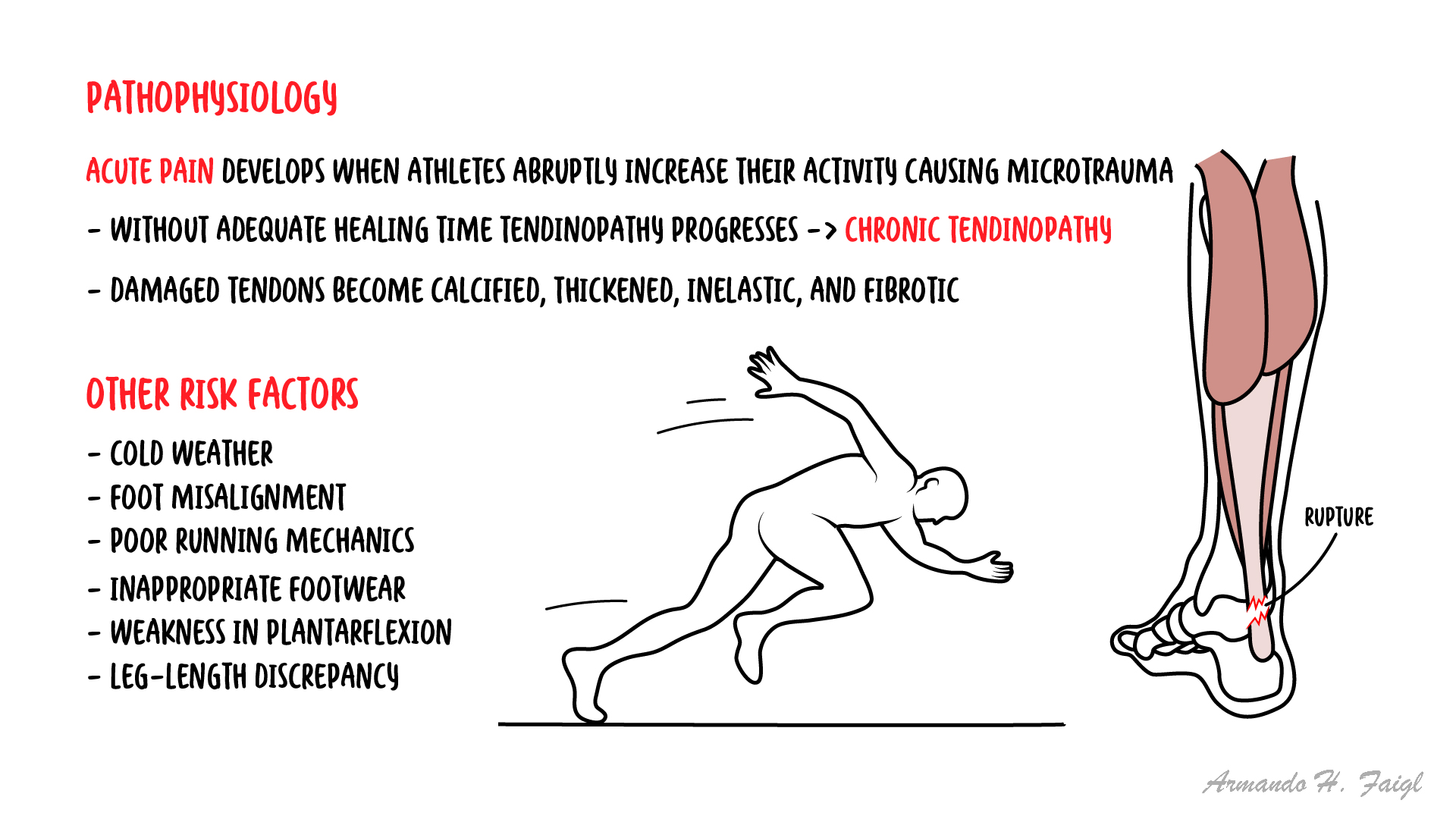
- Repetitive overload → microtears in tendon collagen.
- Failed healing response → tendinopathy (collagen disorganisation, neovascularisation, thickening).
- Acute rupture: sudden eccentric contraction (e.g., push-off, landing) → tendon fibres tear, often in watershed zone.
Tendinopathy = chronic degeneration; rupture = acute overload failure.
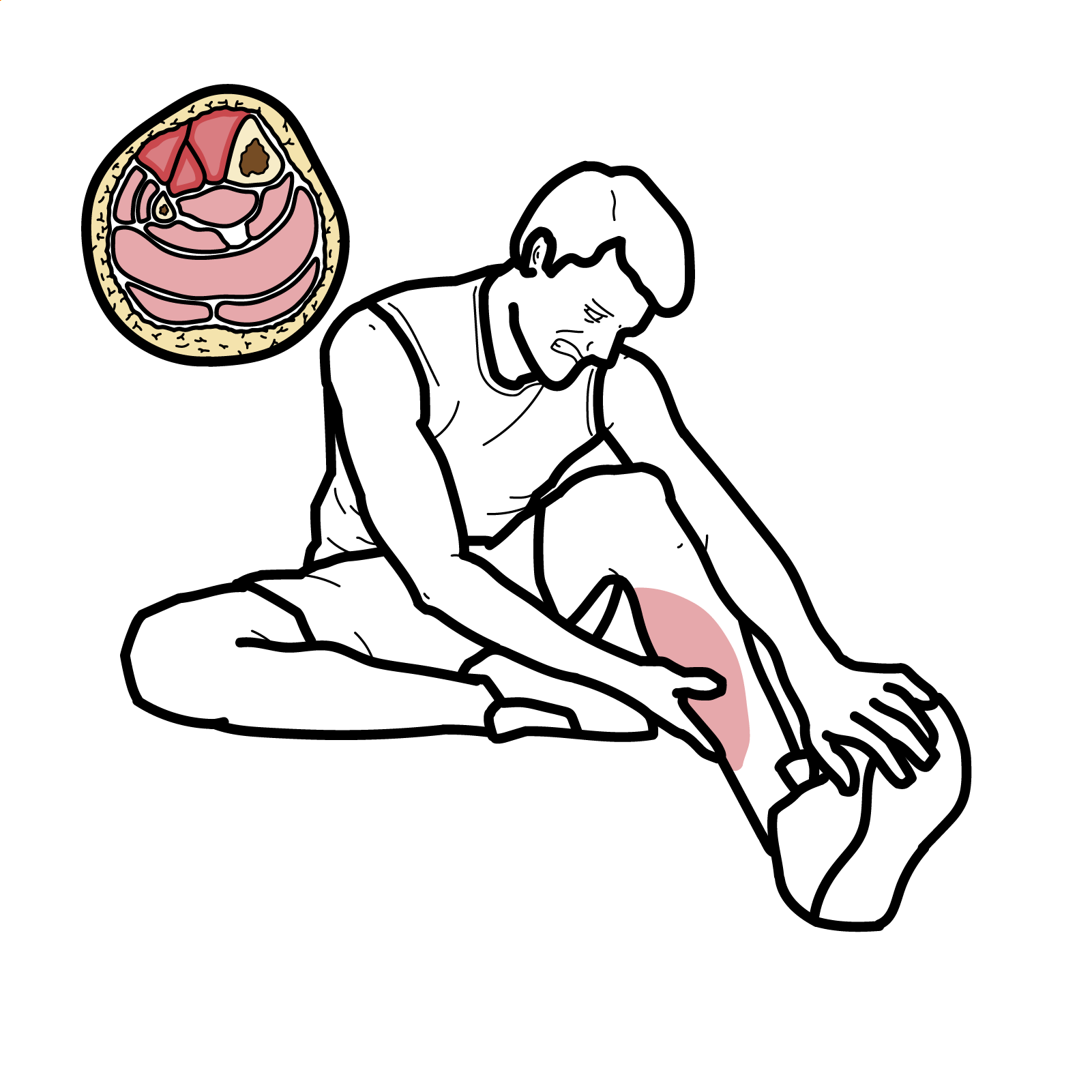
Clinical Manifestations
- Tendinopathy
- Gradual posterior heel pain, worse with activity.
- Stiffness, especially in the morning.
- Local swelling/thickening of tendon.
- Pain on palpation, crepitus sometimes.
- Rupture
- Sudden “pop” or snap in posterior ankle.
- Acute pain, difficulty walking or pushing off.
- Palpable gap in tendon.
- Positive Thompson test (no plantarflexion when calf squeezed).
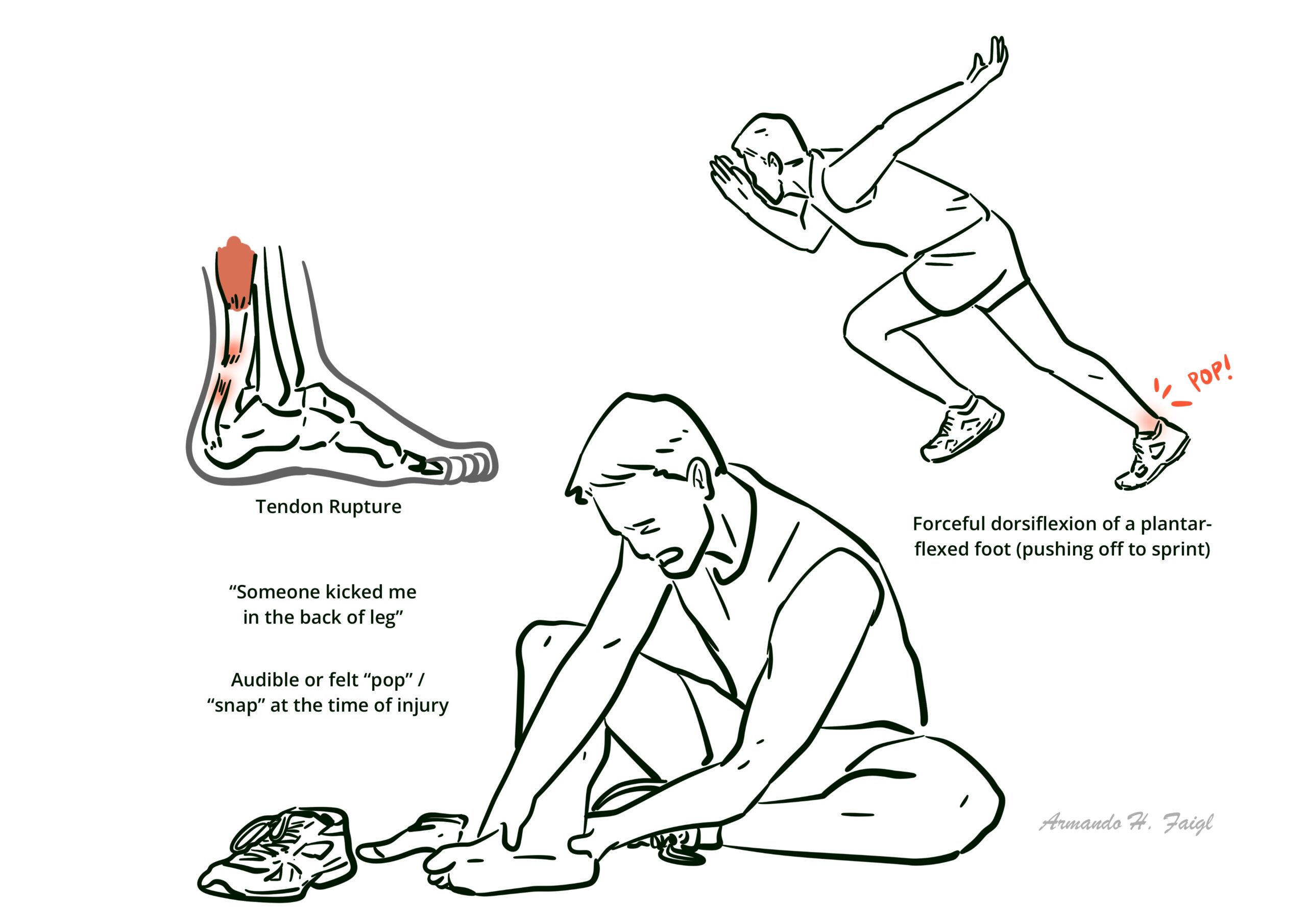

A patient who thinks they’ve been “kicked in the back of the leg” but no one was there likely ruptured their Achilles.
Triad: Sudden “pop” in ankle, Palpable tendon gap, Positive Thompson test.
Diagnosis
- Clinical diagnosis
- Tendinopathy: Ultrasound or MRI shows tendon thickening, hypoechoic areas, neovascularisation.
- Rupture:
- Clinical: palpable gap, positive Thompson test.
- MRI or ultrasound confirms extent, especially for partial ruptures.
Achilles Tendinopathy vs Rupture
| Feature | Tendinopathy | Rupture |
| Onset | Gradual, chronic | Sudden, acute |
| Pain | Activity-related, morning stiffness | Sudden severe pain, may subside quickly |
| Exam | Thickened, tender tendon | Palpable gap, Thompson test + |
| Function | Pain but preserved strength | Loss of push-off, impaired walking |
| Imaging | US/MRI: thickened tendon | US/MRI: complete/partial discontinuity |
Differential Diagnosis
| Condition | Differentiator |
| Plantaris rupture | Pain more medial, intact plantarflexion |
| Retrocalcaneal bursitis | Local swelling, no tendon defect |
| Posterior ankle impingement | Pain with plantarflexion, no tendon abnormality |
Treatment
- Tendinopathy:
- Load modification (reduce aggravating activities).
- Eccentric calf strengthening (Alfredson protocol).
- Heel lifts, orthotics if needed.
- NSAIDs for pain (not disease-modifying).
- Shockwave therapy, PRP injections (mixed evidence).
- Rupture:
- Non-operative (functional rehabilitation):
- Early functional bracing with controlled ankle motion.
- Best in low-demand patients or partial ruptures.
- Operative:
- Surgical repair (open or percutaneous) indicated in young/athletic patients.
- Lower re-rupture rates but higher wound complication risk.
- Non-operative (functional rehabilitation):
- Rehabilitation: Structured progressive loading over 6–12 months.
Eccentric strengthening = gold standard for tendinopathy; surgery vs functional rehab depends on patient profile.
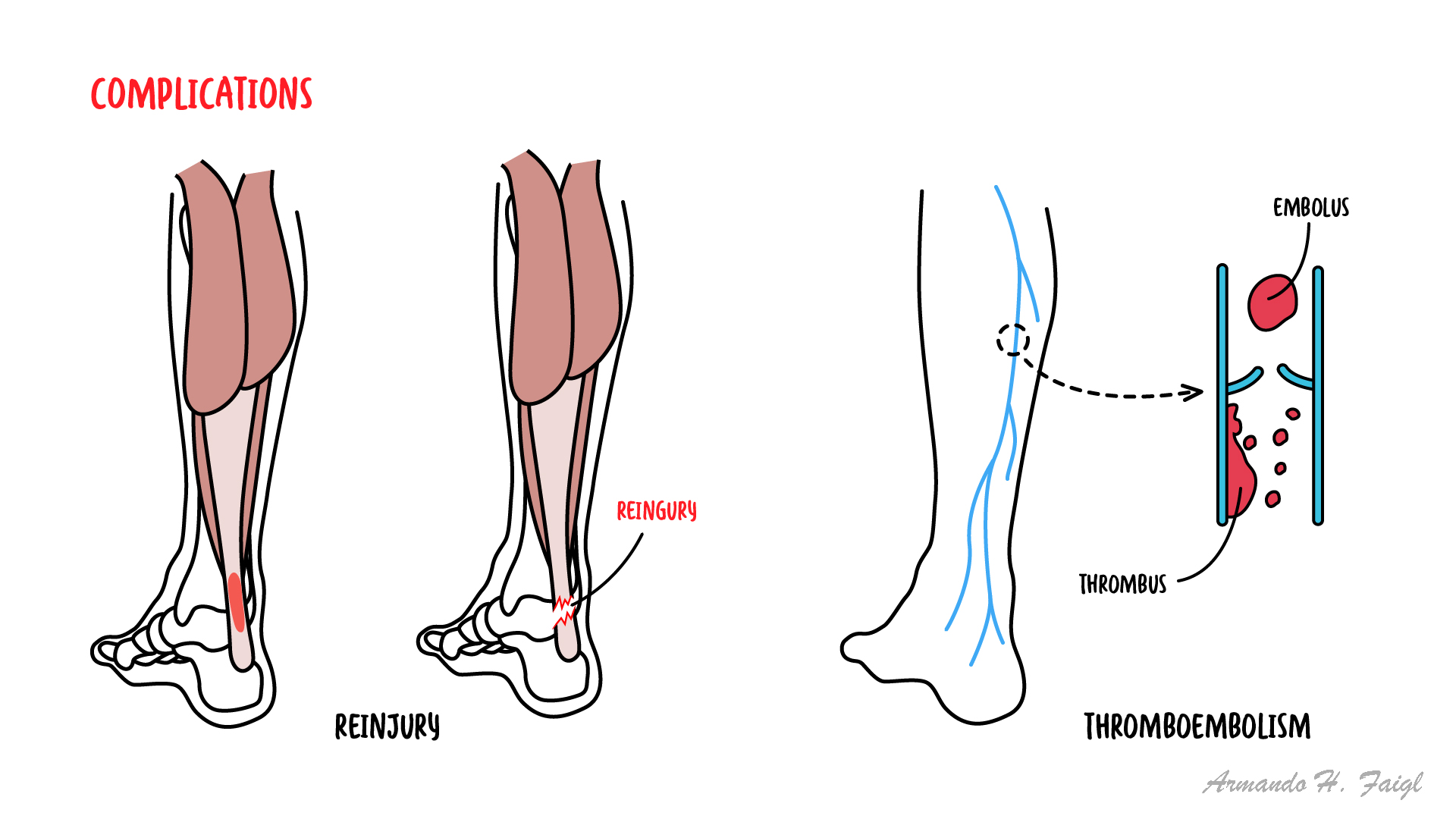
Complications & Prognosis
- Tendinopathy: Chronic pain, functional limitation, rupture risk.
- Rupture:
- Prognosis: Good with rehab, but return to sport may take 6–12 months.
Delayed or missed rupture diagnosis → poor functional outcomes.
References
- Maffulli N, Longo UG, Denaro V. Achilles tendinopathy. Sports Med Arthrosc Rev. 2010;18(1):11–5.
- Soroceanu A, Sidhwa F, Aarabi S, Kaufman A, Glazebrook M. Surgical vs nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis. J Bone Joint Surg Am. 2012;94(23):2136–43.
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360–6.
- Ochen Y, Beks RB, van Heijl M, et al. Operative treatment vs nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364:k5120.
- Kannus P, Jozsa L. Histopathological changes preceding spontaneous rupture of a tendon. J Bone Joint Surg Am. 1991;73(10):1507–25.





Members only discussions coming soon…