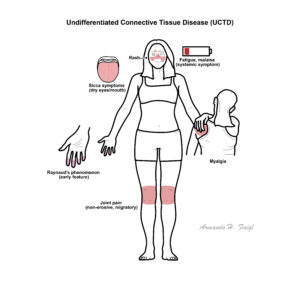
UCTD is a systemic autoimmune disease with features of connective tissue disease (CTD), but does not fulfill classification criteria for any specific CTD such as SLE, Sjögren’s syndrome, systemic sclerosis, or polymyositis. It is a diagnosis of exclusion used for patients with persistent autoimmune features who do not evolve into a defined CTD. Commonly affects women of childbearing age. Estimated prevalence ranges from 20% to 30% of all CTD presentations in early stages.
Definition
UCTD: Autoimmune disease with clinical signs and autoantibodies suggestive of CTD, but not meeting criteria for any defined CTD. Connective Tissue Disease (CTD): A group of autoimmune diseases affecting connective tissues such as skin, joints, and blood vessels.
Mosca M et al. Undifferentiated connective tissue diseases: a review of the literature and proposal for preliminary classification criteria. Clin Exp Rheumatol. 1999;17(5):615–620.
Doria A, Mosca M, Gambari PF, Bombardieri S. Defining unclassified connective tissue diseases: incomplete, undifferentiated, or both? J Rheumatol. 2005;32(2):213–215.
Kinder AJ, et al. Clinical manifestations of undifferentiated connective tissue disease in a large cohort. Arthritis Rheum. 2006;55(3):403–410.














Discussion