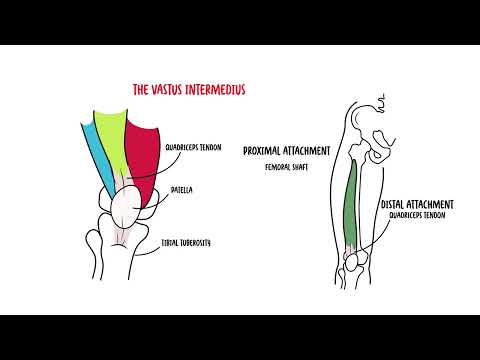
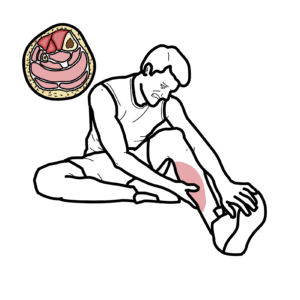
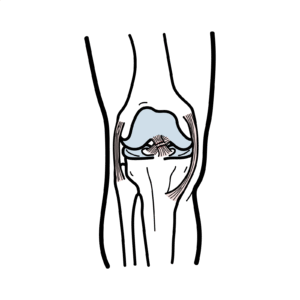
0:00 Patella tendinitis is inflammation and pain over the patella tendon. 0:12 The patella is the largest sesomoid bone in the human body. 0:17 It is located anterior to the knee joint within the tendon of the quadriceps 0:23 muscle, providing 0:24 an attachment point for both the quadriceps tendon and the patella ligament. 0:31 The quadriceps consist of four individual muscles, the rectus femoris, fastest 0:38 lateralis, 0:40 fastest medialis, and fastest intermedius. 0:45 The quadriceps muscle have different origins, but converge and insert onto the 0:50 patella as 0:50 the common quadriceps tendon. 0:53 This tendon then envelopes the patella and inserts onto the tibial tuberosity. 0:59 The portion of the tendon that extends inferior to the patella, the bone, is 1:04 generally referred 1:06 to as the patella tendon. 1:08 Some texts refer to it as the patella ligament. 1:16 The combined action of the quadriceps can generate powerful knee extension, and 1:22 this 1:23 is in part due to the help of the patella tendon, obviously attaching to the t 1:30 ibia. 1:31 In addition to its role in knee extension, the patella tendon provides joint 1:37 stability 1:37 during landing and de-acceleration from running and acts as a passive stabil 1:43 izer of 1:44 the patella bone. 1:46 The patella moves along what's called the trochlea groove during knee extension 1:54 and 1:55 knee flexion, moving up and down this trochlea groove. 2:04 The patella tendon origin usually has a crescent shape, with the medial and 2:11 lateral fascicles 2:12 attached to the patella more proximally than the central fascicles. 2:17 At its insertion on the proximal tibia, the patella tendon fans out, mingling 2:24 distally 2:25 with the fascia of the iliotibial tract or band. 2:36 The mechanism of patella tendonitis is obviously an overuse injury. 2:43 Patella related injuries are very common, especially in jumping sports such as 2:48 basketball 2:48 and volleyball, and sports characterized by rapid acceleration, de-acceleration 2:55 , and 2:55 change of direction. 2:57 That is why patella tendonitis is sometimes referred to as jumpers knee. 3:06 Some risk factors for patella tendonopathy includes core biomechanics, male sex 3:14 , more 3:15 than 20 hours of training per week, previous knee injury, fluoroquinolone use, 3:23 other medications 3:25 also that increases the risk of patella tendonopathy include glucocorticoids, 3:30 aromatase inhibitors, 3:32 and HMG-CoA reductase inhibitors, also known as statins. 3:41 The clinical presentation of patella tendonopathy is really pain localized to 3:46 the inferior 3:47 pole of the patella. 3:49 The patients often point to the spot. 3:52 The pain is load related that increases with the demand on the knee extensors, 3:59 such as 4:00 during jumping and hopping. 4:02 Pain is usually of gradual onset and worse with training. 4:08 There's something called the warm-up phenomenon also, in which the patella 4:12 tendon pain may 4:14 actually decrease during training, but then often the pain is a lot worse after 4:20 training 4:21 or the match the following day. 4:26 Without adequate time to recover, patella tendonitis or tendonopathy can become 4:36 chronic. 4:38 Clinical examination often reveals focal pain in the patella tendon, that is 4:43 worse with 4:44 loading maneuvers like hopping or de-exceleration. 4:49 The single leg decline squat typically causes a lot of pain localized in this 4:56 region in 4:57 early knee flexion. 5:03 Differential diagnosis for patella tendonitis and patella tendonopathy includes 5:09 patello femoral 5:10 pain, also known as runners knee, knee bursitis, or schlata disease, which is t 5:17 ibial tuberosity 5:19 a volgan, sinning larson johansen disease, which is inferior patella apophysis 5:28 a volgan, 5:29 fat pad syndrome, plica syndrome, and quadriceps tendonopathy, which would be 5:37 more located 5:38 superiorly to the patella. 5:45 Investigations The diagnosis is really based on history 5:48 and clinical examination, however, investigations that could be ordered include 5:53 an ultrasound 5:53 in the region which could reveal tendon tears, x-ray as well as MRI if the 5:59 diagnosis is uncertain. 6:05 Treatment includes rice, resting, icing the area, possibly compression and 6:13 elevation early 6:14 on, analgesia used include ibuprofen or neurofen, physiotherapy is important so 6:22 exercise and 6:23 rehabilitation, typically isometric and then dynamic strength exercises, using 6:30 adjuncts 6:30 such as wrapping the knee taping as well as massaging the area if it's tight 6:37 and stiff. 6:38 Injection therapy is also used if the above are not working and this can 6:42 include glucocortic 6:44 cord injection, and some centers also inject the tendon with plasma-rich plate 6:52 lets. 6:53 Surgery is rarely required. 7:00 Complications Complete rupture of the patella tendon rarely occurs, but the 7:05 risk may be 7:05 increased with glucocortic cord injections. 7:12 In summary, we talked about the anatomy of the quadriceps muscle and patella 7:19 tendon specifically. 7:20 We discussed patella tendonopathy, tendonitis, a common disorder in people who 7:26 jump a lot. 7:27 We also explored the differential diagnosis of patella tendopathy and the 7:32 treatment. 7:35 We also explored the treatment of patella tendonopathy, which is the best way 7:41 to do this.