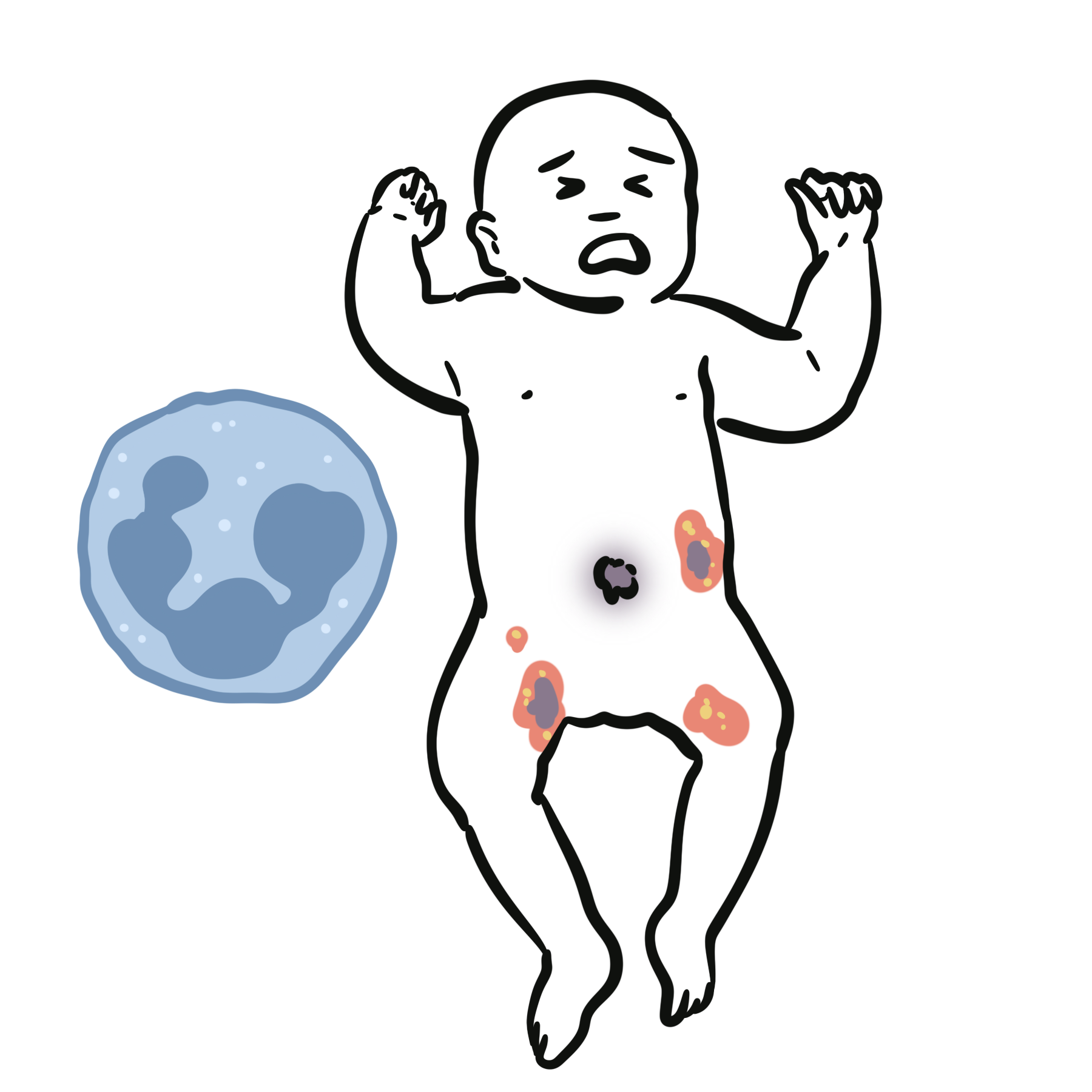
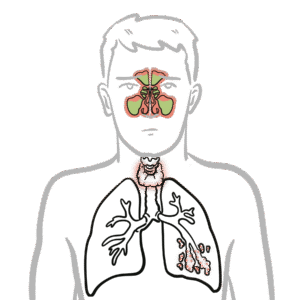
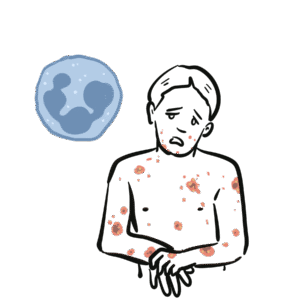
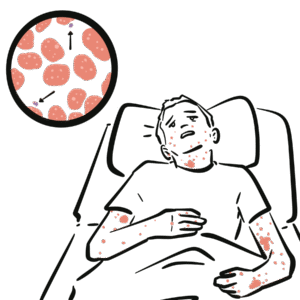
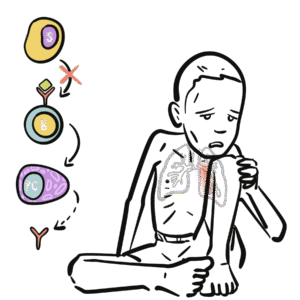
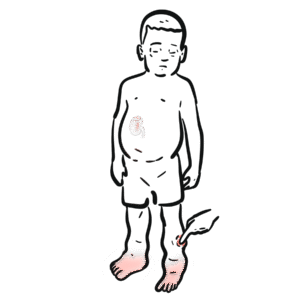
Leukocyte adhesion deficiency (LAD) is a rare primary immunodeficiency characterised by recurrent bacterial and fungal infections, impaired wound healing, and absence of pus formation due to defective leukocyte adhesion and migration. It results from genetic defects in leukocyte integrins or signalling pathways, preventing neutrophil extravasation from blood vessels into tissues. LAD has an estimated incidence of 1 per 100,000–200,000 live births. The most common and severe form is LAD type 1 (CD18/β2 integrin deficiency).
Definition
Integrin (CD18/β2): Cell surface protein mediating firm adhesion of leukocytes to endothelium. Chemotaxis: Directed movement of immune cells toward sites of infection/inflammation. Pus: Accumulation of neutrophils at infection site; absent in LAD due to failure of migration. Omphalitis: Infection of the umbilical stump; common early presentation in LAD.
Anatomy & Physiology
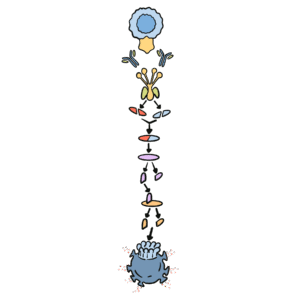
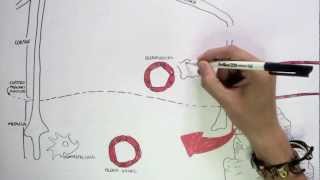
Normal neutrophil migration:
Rolling (selectins) → adhesion (integrins: LFA-1/CD18) → diapedesis → chemotaxis.
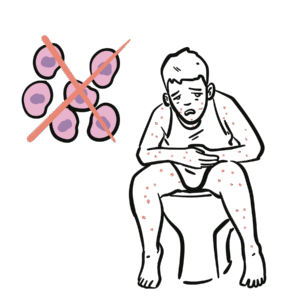
In LAD: defective adhesion (type 1), defective rolling (type 2), or defective signalling (type 3) → neutrophils cannot exit bloodstream.
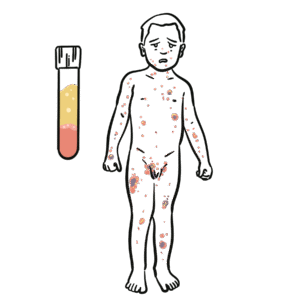
Neutrophil count normal/high in blood, but no neutrophils at infection site.
Neutrophilia + recurrent infections without pus strongly suggests LAD.
Aetiology
LAD-1: AR mutation in ITGB2 gene (β2 integrin/CD18 deficiency).
LAD-2: AR defect in GDP-fucose transporter → impaired selectin ligand synthesis → defective rolling.
LAD-3: AR defect in KINDLIN-3 → impaired integrin activation affecting leukocytes and platelets.
Prognosis: poor without HSCT in severe LAD-1 and LAD-3; supportive care may allow survival in milder cases.
Most severe cases die in early childhood without transplant.
References
Etzioni A, Harlan JM. Cell adhesion molecules in leukocyte adhesion deficiency. Semin Hematol. 2000;37(4):373–81.
Almarza Novoa E, Kasbekar S, Thrasher AJ, et al. Leukocyte adhesion deficiency: Molecular basis, clinical presentation, and therapeutic approaches. Front Immunol. 2018;9:1031.
Anderson DC, Springer TA. Leukocyte adhesion deficiency: An inherited defect in the Mac-1, LFA-1, and p150,95 glycoproteins. Annu Rev Med. 1987;38:175–94.
Fischer A, Notarangelo LD, Neven B, et al. Primary immunodeficiency diseases: An update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 2020;40:24–64.
Kinashi T. Intracellular signalling controlling integrin activation in lymphocytes. Nat Rev Immunol. 2005;5(7):546–59.







Discussion