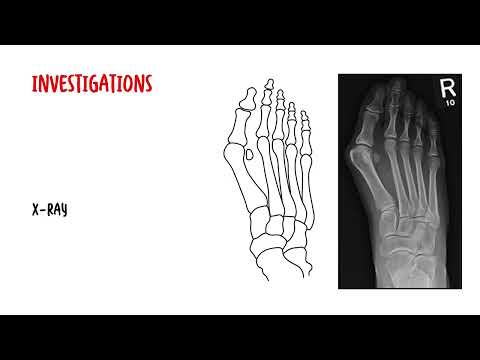
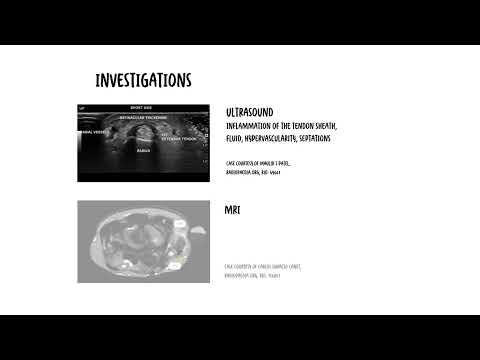
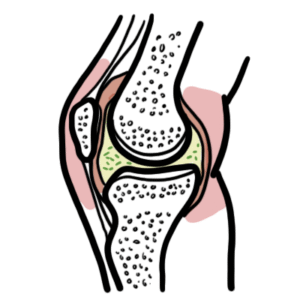
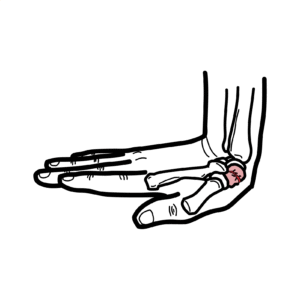
0:00 Hello, in this video, we're going to talk about septic arthritis. 0:08 This is an introduction and overview. 0:11 With any monoarthritic presentation, it is important to rule out septic 0:17 arthritis, as 0:18 this can cause irreversible damage to the joint. 0:22 Common symptoms of septic arthritis include fever, monoarthritis, which means 0:29 one inflamed 0:30 joint. 0:32 Inflammation of the joint is characterized by warmth, redness, erythema, pain, 0:38 and decreased 0:39 in function or range of movement. 0:43 The person presenting with an inflamed joint requires a thorough history and 0:49 examination. 0:50 For septic arthritis, the main causative agents include staphylococcus aureus, 0:56 group A streptococcus, 0:59 and nseria gonorrhea, which is a sexual transmitted bacteria. 1:05 A quick recap of the pathogenesis of septic arthritis, here is an inflamed 1:14 joint. 1:15 A skin infection, such as that from staphylococcus aureus, can disseminate into 1:21 the joint causing 1:22 septic arthritis. 1:25 Osteomyelitis, which is inflammation infection of the bone marrow, usually 1:29 caused by staphylococcus 1:30 aureus, again, can locally invade the joint, causing septic arthritis. 1:37 Upper respiratory tract infections or lower respiratory tract infections from 1:43 group A 1:43 streptococcus can hematogenously go to the bone causing osteomyelitis, which 1:50 then can 1:51 lead to septic arthritis. 1:55 Alternatively, there can also be an STI from nseria gonorrhea that can dissemin 2:01 ate into 2:02 the joint causing septic arthritis. 2:07 Procedures such as injections to the joint space can introduce bacteria into 2:11 the joint 2:12 causing septic arthritis. 2:14 Further, it's important to consider surgery as a cause of septic arthritis 2:18 during surgery, 2:20 bacteria may enter the joint from skin or from aseptic techniques. 2:25 Again, with monoarthritis, any monoarthritic presentation, it's important to 2:30 rule out 2:31 septic arthritis. 2:33 It is a surgical emergency with greater than 24 hours leading to irreversible 2:39 joint damage. 2:41 Negations to be performed in a person presenting with monoarthritis include a 2:46 full blood count, 2:48 C-reactive protein, ESR to check for signs of inflammation and infection. 2:56 A joint aspiration is usually indicated for a monoarthritic presentation. 3:02 The joint aspiration will also need to be cultured microscopy, culture, and 3:08 sensitivity. 3:09 It's important to also do blood cultures if you suspect systemic infections or 3:14 bacteremia. 3:16 Also perform electrolyte urea creatinine and glucose. 3:20 Finally, imaging including ultrasound and x-ray can also be done. 3:26 X-ray may reveal subluxation or dislocation of the joint, and there is joint 3:30 space widening 3:31 because of the swelling and inflammation occurring within the joint itself. 3:38 After performing the investigations, notably cultures and joint aspiration, 3:42 administration 3:43 of broad-spectrum antibiotics is priority. 3:47 Then, surgical emergency is needed involving joint drainage, usually joint 3:54 aspiration, 3:55 atheroscorpic drainage, or open drainage. 4:00 Once cultures have come back and results are obtained from the joint aspiration 4:05 or blood 4:06 cultures, antibiotics can be tailored towards the causative agent. 4:11 These antibiotics are given typically two weeks with IV, then changing to oral 4:17 antibiotics 4:18 for four weeks. 4:20 Follow-up and monitoring is also important throughout this whole time.