↓↑Potassium (Hyperkalaemia and Hypokalaemia)

Potassium (K+) is an important ion in the body. K+ is found mainly intracellularly (inside the cells) whereas sodium (Na+) is found extracellularly (outside the cells).
Therefore:
As the pH rises , K+ is shifted intracellularly and the serum levels falls; conversely when serum pH decreases, intracellular K+ shits extracellularly into the vascular space and so the serum level increases. This is because H+ and K+ are both positive and it is important to have normal +ions levels in the serum to maintain a gradient across the cell membrane to maintain the excitability of nerve and muscle cells, including the myocardium.
Management – pharmacological
| Pharmacology Calcium Gluconate is a myocardium stabiliser and is cardioprotective. Side effects: Bradycardia, hypotension and peripheral vasodilation. |
| Pharmacology Calcium Resonium is a large insoluble molecule that binds to K+ in the large intestine, where it is excreted in faeces. Side effects: |
| MANAGEMENT OF HYPERKALAEMIA DEPENDING ON SEVERITY | ||
| Mild | Moderate | Severe |
| Calcium Resonium | IV Frusemide | IV Frusemide |
| Calcium Resonium | Calcium gluconate/Calcium chloride | |
| Insulin + Dextrose/N.Saline | Insulin + Dextrose/N.Saline | |
| Salbutamol | Salbutamol | |
Defined as potassium <3.5mmol’L
Management – nonpharmacological
Management – pharmacological
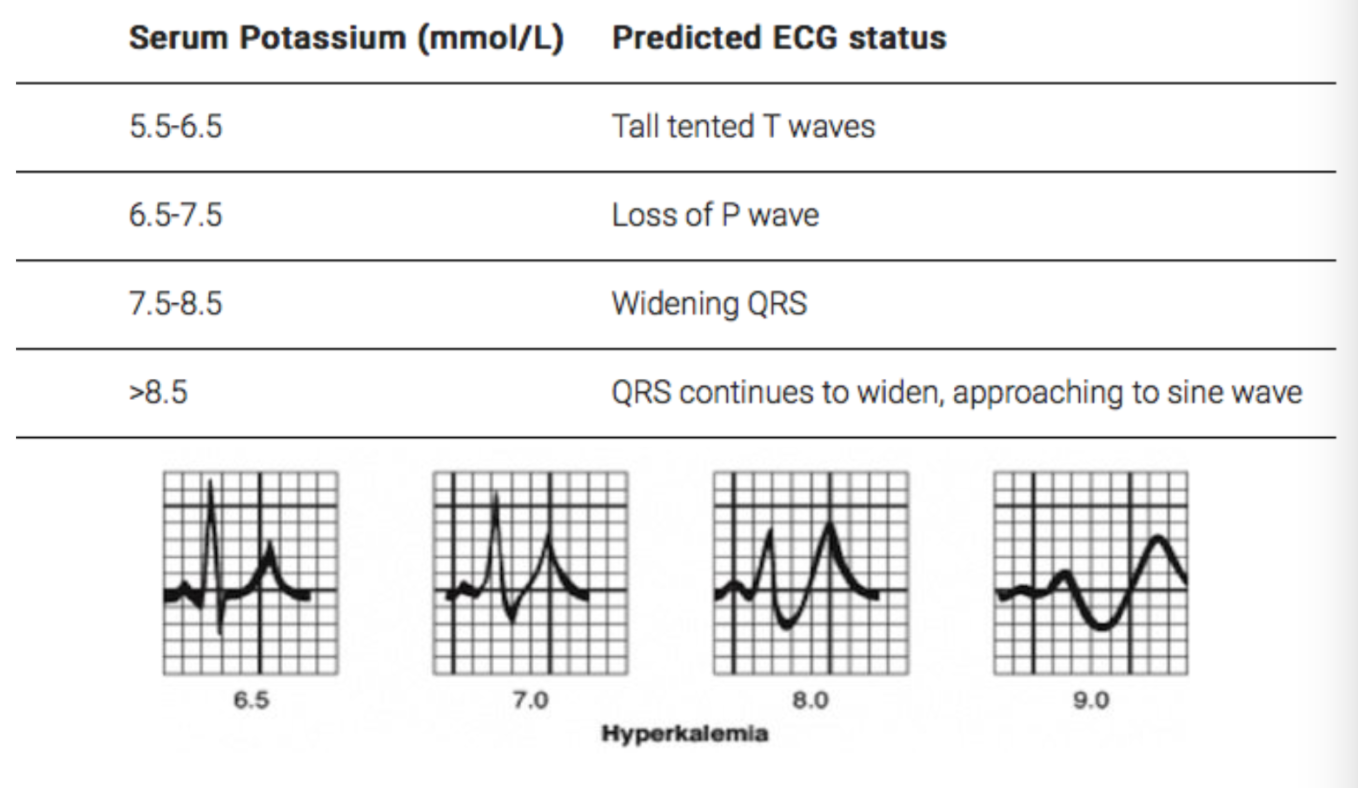
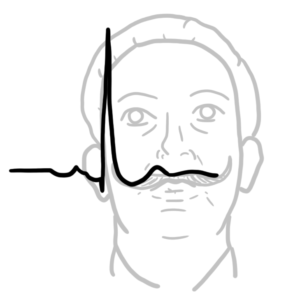
ECG findings

















Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion