

Addison's Disease
Overview
Addison’s disease is a disease characterised by adrenal insufficiency. Adrenal insufficiency results in a decrease of the adrenal gland hormones: mineralocorticoids, glucocorticoids and to an extent androgens. There are many causes of addison’s disease. The most common cause in the developed world is autoimmune (approximately 70% cases). Signs and symptoms of adrenal sufficiency don’t really occur until 90% of adrenal function is lost.
Definition
Adrenal insufficiency: Adrenal insufficiency results from inadequate adrenocortical function and may be due to destruction of the adrenal cortex (primary or Addison’s disease) or to disordered pituitary and hypothalamic function (secondary).
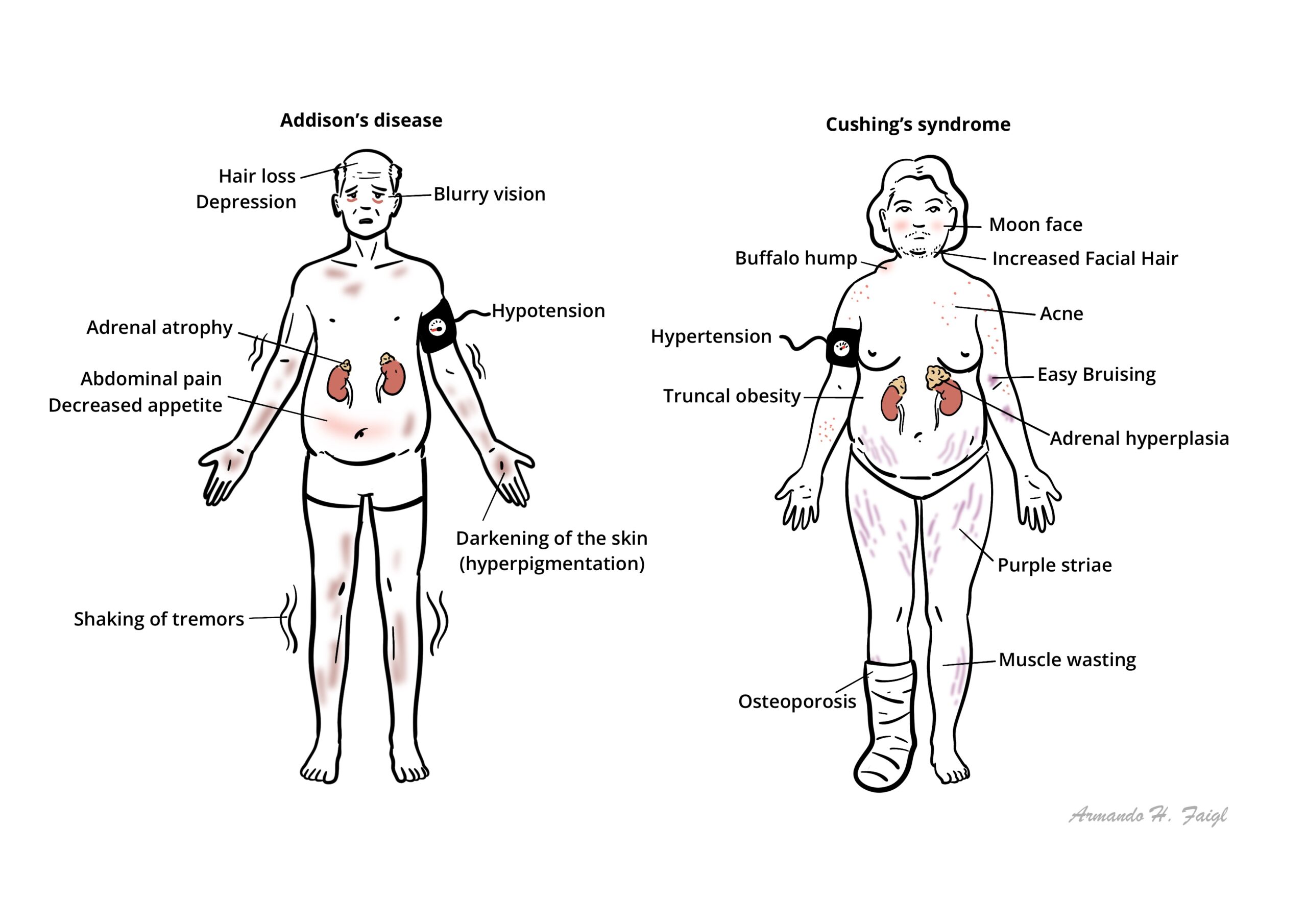
Addison’s Disease: Primary adrenal sufficiency independent of hypothalamic, pituitary dysfunction
Cushing’s Disease: Hypercortisolemia from an ACTH-secreting pituitary tumor (ACTH Dependent).
Adrenal Glands Anatomy & Physiology
Anatomy
- The normal adrenal glands weigh 4–5 g.
- The cortex represents 90% of the normal gland and surrounds the medulla.
- The arterial blood supply arises from the renal arteries, aorta, and inferior phrenic artery.
- Venous drainage occurs via the central vein into the inferior vena cava on the right, and into the left renal vein on the left.
- Three layers of the adrenal glands
- Zona fasiculata
- Zona glomerulosa
- Zona Reticularis
Physiology
- Glucocorticoids (zona fasciculata)
- Mineralcorticoids (zona glomerulosa)
- Androgens (zona reticularis and zona fasciculata)
Aetiology
There are many causes of Addison’s Disease
- Autoimmune (70%)
- Malignancy (metastatic, lymphoma)
- Infiltration (amyloid, haemochromatosis)
- Infection
- Vascular haemorrhage
- Infarction
- Adrenoleucodystrophy
- Congenital adrenal hyperplasia
- Iatrogenic (Adrenalectomy, Drugs)
Pathophysiology
Adrenal gland destruction or dysfunction occurs from a disease process that usually involves all three zones of the adrenal cortex, resulting in inadequate glucocorticoid, mineralocorticoid, and androgen secretion. Autoimmunity is the main etiologic factor.
The manifestations of insufficiency do not usually appear until at least 90% of the gland has been destroyed and are usually gradual in onset, with partial adrenal insufficiency leading to an impaired cortisol response to stress, and the features of complete insufficiency occurring later.
Acute adrenal insufficiency may occur in the context of acute septicemia (e.g., meningococcal or hemorrhage).
Mineralocorticoid deficiency leads to reduced sodium retention and hypotension with ↓ intravascular volume, in addition to hyperkalemia due to ↓ renal potassium and hydrogen ion excretion.
Androgen deficiency presents in women with reduced axillary and pubic hair and reduced libido. (Testicular production of androgens is more important in men.)
Lack of cortisol negative feedback increases CRH and ACTH secretion. An increase in other POMC-related peptides leads to skin pigmentation and other mucous membranes.
Clinical Manifestations
Acute
- Adrenal Crisis (Life-threatening)
Acute Adrenal insufficiency (Adrenal Crisis) is commonly caused when patients who are on long term glucocorticoids suddenly stop or do not increase dosage during febrile illness.
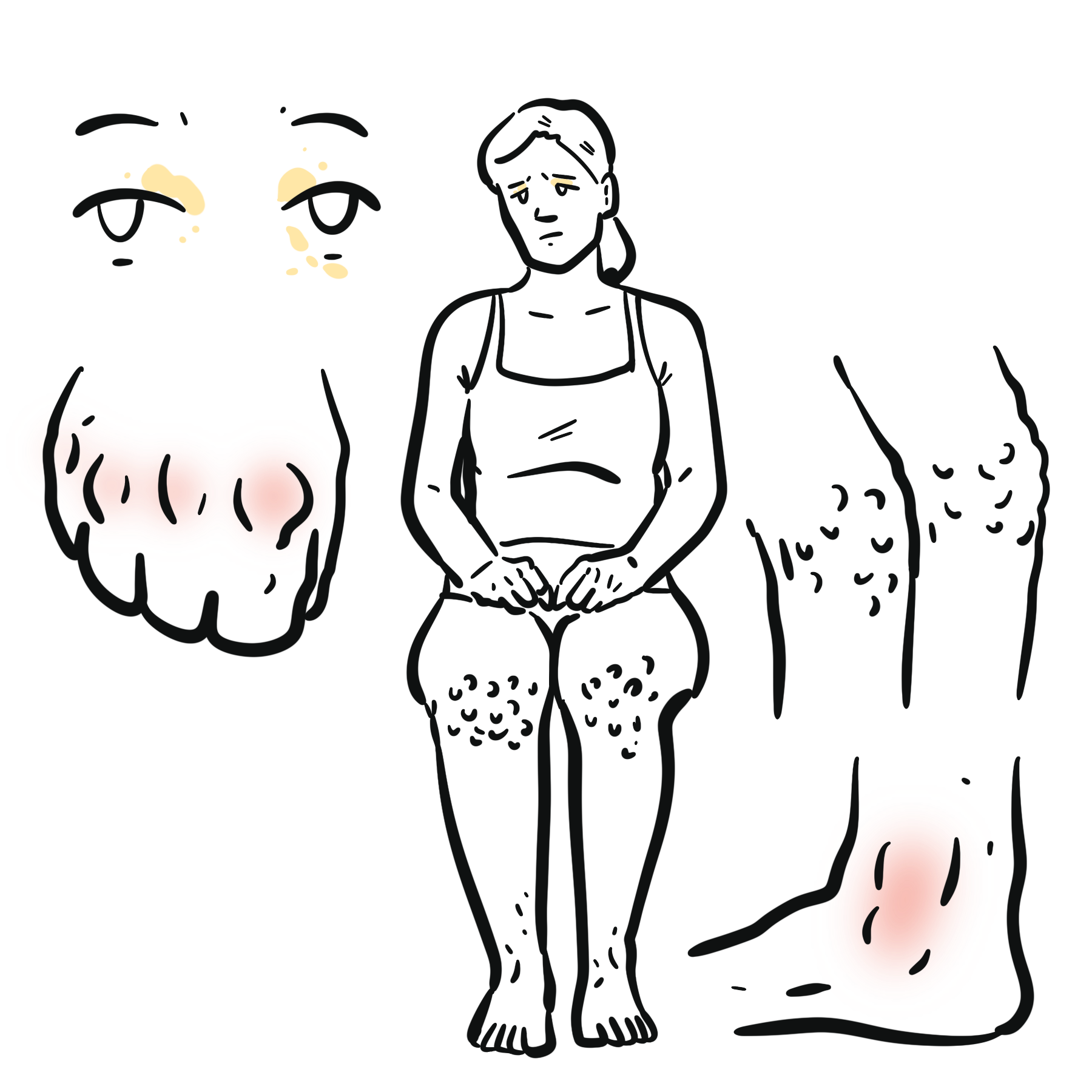
General presentation (Chronic)
- Anorexia and weight loss (>90%)
- Tiredness
- Weakness—generalized, no particular muscle groups
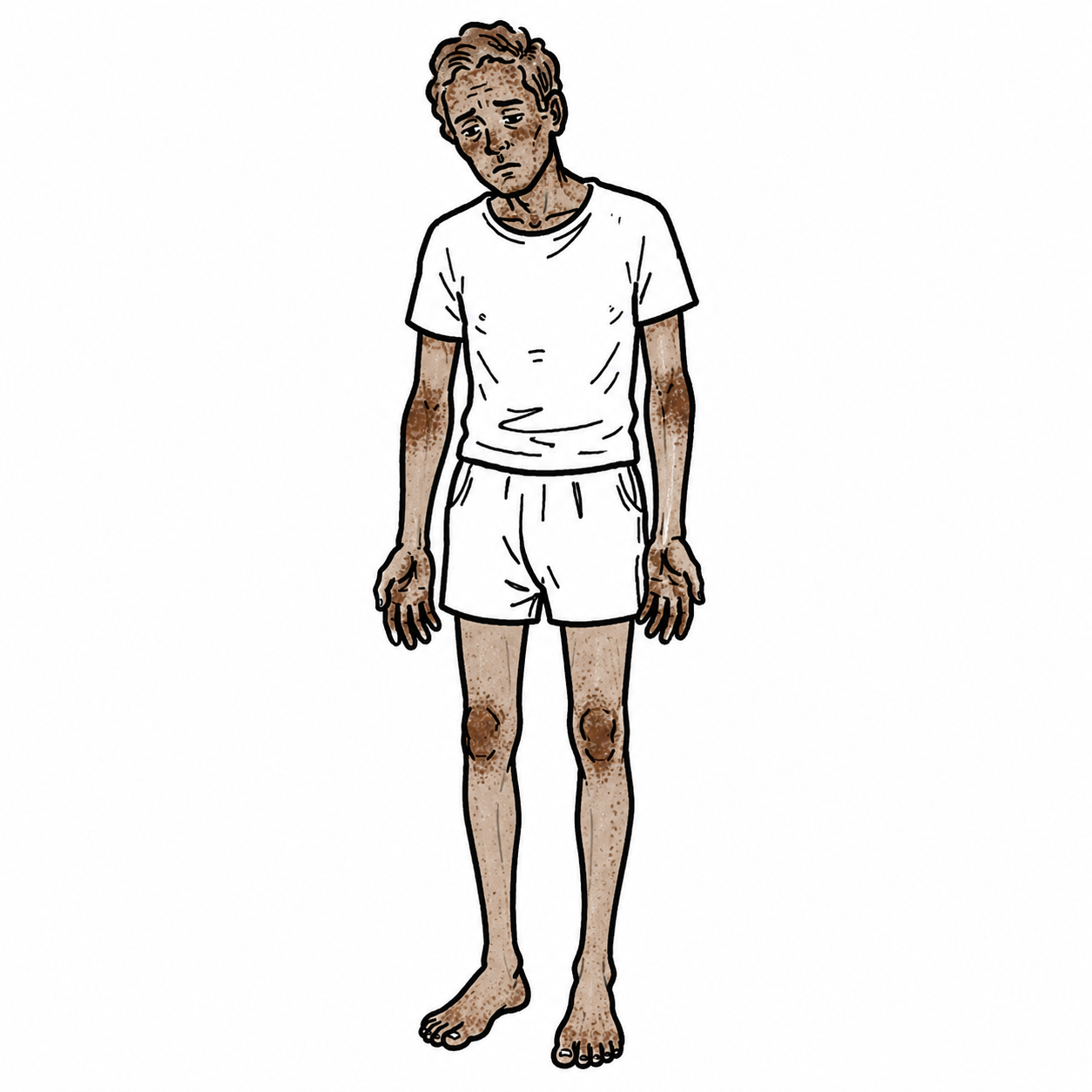
- Pigmentation—generalized, but most common in light-exposed areas and areas exposed to pressure (elbows and knees, and under bras and belts); mucosa and scars acquired after onset of adrenal insufficiency. Look at palmar creases in Caucasians.
- Dizziness
- GI symptoms—nausea and vomiting, abdominal pain, diarrhea
- Arthralgia and myalgia
- ↓ Axillary and pubic hair and reduced libido in women
Clinical Examination
- Skin pigmentation (sun exposed areas, mucosal surfaces)
- Cachexia
- Loss of body hair
- Low grade fever (rare)
- Postural hypotension
- Signs of dehydration
Investigations
Initial blood tests
- 8–9 am serum cortisol with plasma ACTH
- UEC: hyponatraemia, hyperkalaemia, raised urea
- Blood glucose: may show hypoglycaemia
- FBC: possible anaemia or eosinophilia
Morning cortisol interpretation:
- <150 nmol/L: adrenal insufficiency likely
- 150–300 nmol/L: indeterminate
- >300 nmol/L: adrenal insufficiency unlikely
- Interpret according to the local cortisol assay.
Short Synacthen test—confirmatory test
- Measure cortisol before and 30–60 minutes after 250 micrograms synthetic ACTH
- Inadequate cortisol rise confirms adrenal insufficiency; the traditional peak threshold is approximately <500 nmol/L, but this is assay-dependent.
Differentiate primary from secondary disease
- Primary Addison’s: low cortisol with markedly elevated ACTH
- ACTH >2 times the upper reference limit supports primary adrenal insufficiency.
In Secondary Adrenal Insufficiency there is ↓Serum Cortisol and ↓ACTH.
Mineralocorticoid assessment
- Plasma renin: elevated
- Aldosterone: low
Determine cause
- 21-hydroxylase adrenal antibodies: autoimmune Addison’s
- Screen associated autoimmune disease: TFTs, glucose/HbA1c ± coeliac serology
- CT adrenal glands if antibodies negative or malignancy, haemorrhage, infection or infiltration suspected
- Consider tuberculosis, HIV or fungal investigations according to risk factors.
- Hyperthyroidism such as Graves Disease
- Anorexia Nervosa
- Adrenal suppression due to long-term corticosteroids (for example patients with some rheumatological conditions will be on long-term corticosteroids)
- Haemochromotosis
Schmidt syndrome Addison’s Disease and Autoimmune hypothyroidism.
Carpenter Syndrome Addison’s Disease, Autoimmune hypothyroidism and/or Type 1 diabetes mellitus.
Treatment
- Glucocorticoid replacement
- Mineralocorticoid replacement
- Fludrocortisone usually 50–100 micrograms once daily, adjusted to symptoms, blood pressure, electrolytes and renin.
- Maintain adequate salt and fluid intake; avoid unnecessary salt restriction.
- Monitor weight, lying/standing BP, electrolytes, symptoms and signs of steroid over- or under-replacement.
Patient education
- Never abruptly stop glucocorticoid replacement.
- Increase hydrocortisone during fever, infection, trauma, surgery or other major physiological stress.
- During significant illness, use at least 40 mg hydrocortisone daily in divided doses until recovered.
- Provide:
- Written sick-day plan
- Steroid emergency card/medical-alert identification
- Emergency 100 mg IM hydrocortisone kit
- Training for the patient and family.
Dehydroepiandrosterone (DHEA) is an abundant circulating adrenal androgen with a production rate of 25–50 mg/day. Its levels undergo a progressive decline with ↑ age, and there has been interest in its physiological role.
Patient education is the key to successful management. Must be taught never to miss a dose, encouraged to wear a Medic Alert bracelet and every patient should know how to double the dose of glucocorticoid during febrile illness and to get medical attention if unable to take the tablets because of vomiting.
Complications & Prognosis
- Treatment related Hypertension
- Cushing’s Syndrome
- Osteopenia → Osteoporosis
- Adrenal crisis
Adrenal Crisis
- Definition: acute, life-threatening cortisol deficiency causing hypotension and potential shock.
- Usually occurs in known or undiagnosed adrenal insufficiency during physiological stress.
Common triggers
- Infection or sepsis
- Vomiting or diarrhoea
- Surgery, trauma or severe illness
- Missed or abruptly stopped corticosteroids
- Inadequate stress-dose steroids
- Severe weakness, fatigue or collapse
- Hypotension, postural dizziness or shock
- Nausea, vomiting, abdominal pain or diarrhoea
- Dehydration and fever
- Confusion, reduced consciousness or coma
- Hypoglycaemia
- Hyponatraemia
- Hyperkalaemia in primary adrenal insufficiency
- Hyperpigmentation may indicate underlying Addison’s disease
Treatment
- Do not wait for investigation results.
- Hydrocortisone 100 mg IV or IM immediately.
- Then hydrocortisone 200 mg over 24 hours IV, or 50 mg IV/IM every 6 hours.
- Give 1 L 0.9% sodium chloride IV rapidly, then further fluids according to BP, urine output and electrolytes.
- Give IV dextrose if hypoglycaemic.
- Monitor BP, pulse, glucose, sodium and potassium.
- Identify and treat the precipitating cause, commonly infection, vomiting/diarrhoea, trauma, surgery or missed steroids.
- Convert to oral sick-day dosing once haemodynamically stable and able to absorb oral medication.
References
- Bornstein SR, Allolio B, Arlt W, Barthel A, Don-Wauchope A, Hammer GD, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(2):364–389. doi:10.1210/jc.2015-1710.
- Husebye ES, Pearce SH, Krone NP, Kämpe O. Adrenal insufficiency. Lancet. 2021;397(10274):613–629. doi:10.1016/S0140-6736(21)00136-7.
- Rushworth RL, Torpy DJ, Falhammar H. Adrenal crisis. N Engl J Med. 2019;381(9):852–861. doi:10.1056/NEJMra1807486.
- Arlt W; Society for Endocrinology Clinical Committee. Society for Endocrinology endocrine emergency guidance: emergency management of acute adrenal insufficiency (adrenal crisis) in adult patients. Endocr Connect. 2016;5(5):G1–G3. doi:10.1530/EC-16-0054.
- National Institute for Health and Care Excellence. Adrenal insufficiency: identification and management. NICE guideline NG243. London: NICE; 2024.







Members only discussions coming soon…