Anterior cruciate ligament (ACL) tear is one of the most common knee injuries, particularly in young athletes involved in pivoting sports (soccer, basketball, skiing). ACL injuries account for ~50% of all knee ligament injuries, with an incidence of ~68 per 100,000 annually, more common in females due to anatomical and biomechanical risk factors. ACL tears cause instability, impaired performance, and predispose to early osteoarthritis if untreated.
Definition
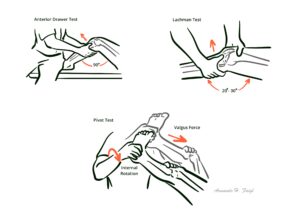
ACL: Intra-articular, extrasynovial ligament preventing anterior tibial translation and providing rotational stability. Pivot shift: Sudden anterior subluxation of tibia during rotation; clinical sign of ACL deficiency. Hemarthrosis: Acute intra-articular bleeding causing rapid knee swelling after ligament tear. Non-contact injury: Injury mechanism where no direct trauma occurs, often from cutting/pivoting movements.
Anatomy & Physiology
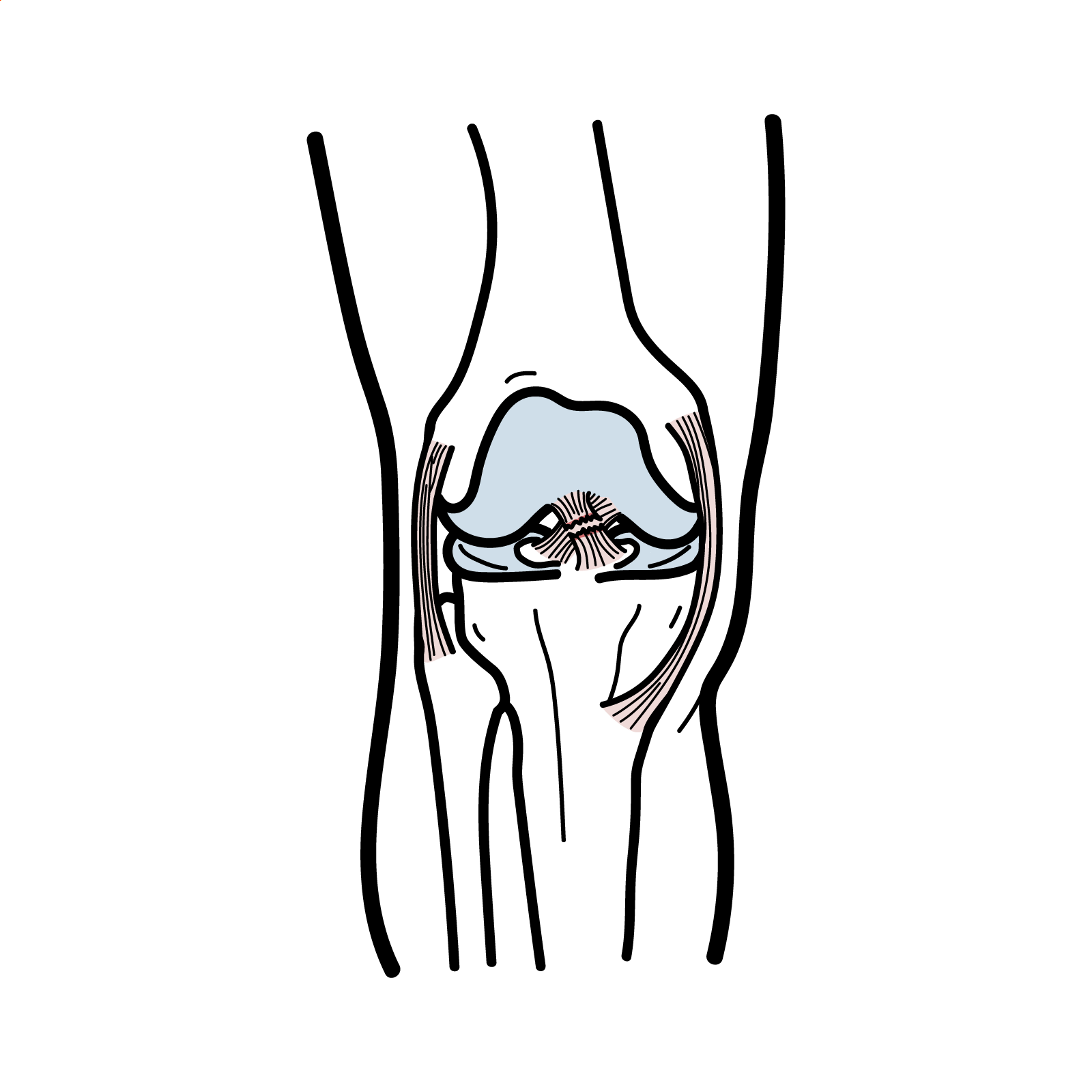
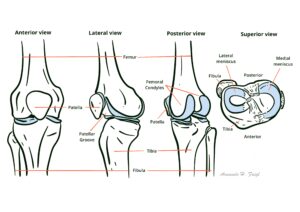
ACL origin: Posterior aspect of lateral femoral condyle.
Insertion: Anterior intercondylar area of tibial plateau.
Function: Restricts anterior translation of tibia relative to femur; stabilises knee during rotation and cutting movements.
Bundles: Anteromedial (tight in flexion) and posterolateral (tight in extension).
This image series is only available to members
ACL is the primary restraint to anterior tibial displacement.
High return to sport but increased long-term OA risk.
Even with reconstruction, ACL injury predisposes to OA.
References
Griffin LY, Albohm MJ, Arendt EA, et al. Understanding and preventing noncontact ACL injuries. Am J Sports Med. 2006;34(9):1512–32.
van Eck CF, Schkrohowsky JG, Working ZM, et al. Clinical examination in the diagnosis of ACL tears: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):1989–96.
Frobell RB, Roos HP, Roos EM, et al. Treatment for acute ACL tear: 5-year outcome of the randomized controlled trial. N Engl J Med. 2010;363:331–42.
Filbay SR, Grindem H. Evidence-based recommendations for rehabilitation after ACL reconstruction. Curr Rev Musculoskelet Med. 2019;12(2):289–96.
Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of ACL tears and reconstruction: a 20-year population-based study. Am J Sports Med. 2016;44(6):1502–7.














Discussion