Alzheimer’s Disease
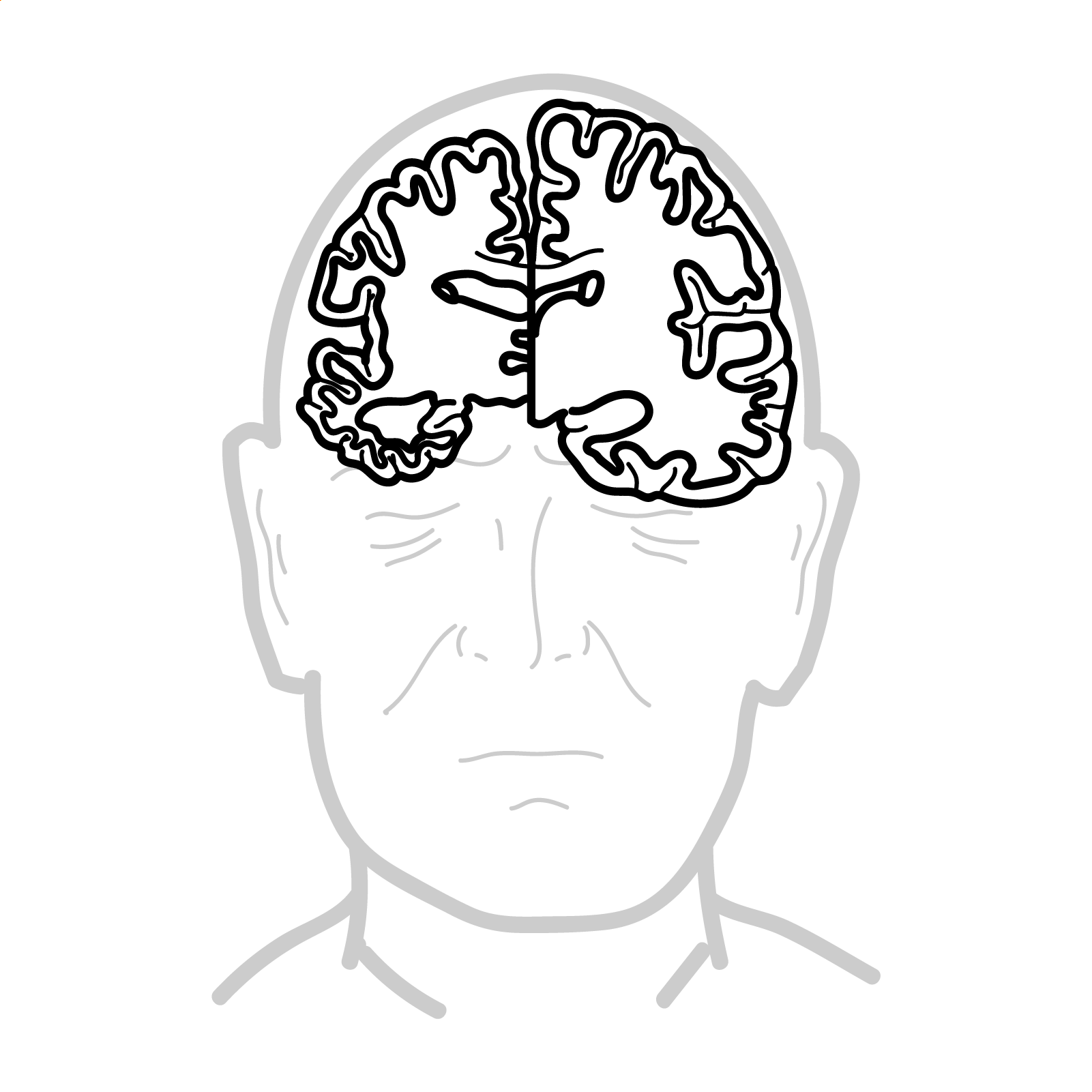

Alzheimer disease is characterised by an insidious onset of symptoms with initial forgetfulness progressing over time to profound memory impairment with accompanying dysphasia, dyspraxia and personality change.
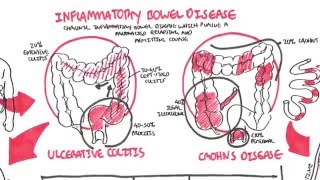
Dementia: Clinical syndrome that is characterised by a progressive deterioration in cognition with resulting decline in function.
Alzheimer disease: Characterised by an insidious onset of symptoms with initial forgetfulness progressing over time to profound memory impairment with accompanying dysphasia, dyspraxia and personality change.
Vascular dementia: Usually starts suddenly and will be accompanied by focal neurological signs with imaging evidence of cerebrovascular disease. Many patients with vascular dementia have evidence of atherosclerotic disease elsewhere.
Frontotemporal lobe dementia (pick’s disease): Selective brain atrophy involving the frontal and temporal lobes, requiring brain magnetic resonance imaging for accurate diagnosis. Clinically, these diseases present chiefly as progressive aphasia or as disintegration of personality and behaviour that may be misdiagnosed as a psychiatric disorder
Lewy body Dementia: Considered the second most common cause of dementia in the elderly after Alzheimer’s disease. DLB is a progressive neurological disorder characterized by core features of cognitive impairment, psychosis and Parkinsonism.
Major dementia syndromes
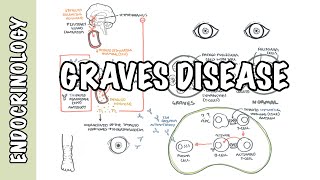
Neuron Anatomy
It has been estimated that up to one third of AD cases worldwide might be attributable to modifiable risk factors such as diabetes, midlife hypertension, and physical inactivity.
Memory impairment:
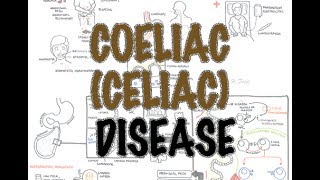
Mini-mental state examination (MMSE)
Physical signs:
Consider other medical causes of memory impairment including hypothyroidism, B group vitamin deficiencies, sleep apnoea, neurosyphilis, cerebral space occupying lesions and normal pressure hydrocephalus.
| Difference between Dementia and Delirium | ||
| Dementia | Delirium | |
| Onset | Sub-acute | Acute |
| Conscious level | Normal | Fluctuates |
| Hallucinations | Late event | Common |
| Agitation/agression | Uncommon until late | Common |
| Thought form | Poverty of thought late | Flight of ideas |
| Memory | Slow decline | Poor |
| DIFFERENTIAL DIAGNOSIS OF ALZHEIMERS | |||
| Alzeihmers Disease | Wernicke-Korsakoff | Picks Disease (FTD) | |
| Early Symptoms | Memory loss | Confusion most common, followed by staggering gait and ocular problems | Apathy, poor judgement/insight, aphasia |
| Onset | Gradual | Days-weeks | Gradual |
| Aetiology | Neurodegeneration | B1 deficiency relatedto alcohol and malnutrition | Neurodegeneration |
| Mental status | Episodic memory loss | Disorientation, minimal spontaneous speech, inattention | Frontal/executive function, language |
| Neuropsychiatry | Initially normal | Apathetic, lack of motivation and insight | Apathy, disinhibition, hyperorality, euphoria, depression. |
| Neurology | Initially normal | Confusion, ataxia, nystagmus | Progressive supranuclear palsy/cortical basal degeneration, vertical gaze palsy, dystonia |
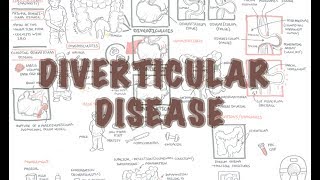
| Imaging | Hippocampal and entorhinal cortex atrophy | Periventricular punctate haemorrhages affecting gray matter | Frontal and/or temporal atrophy |
Cognitive Testing Cognitive tests are vital in the diagnosis of dementia and are often used to differentiate between types of dementia. They can also be used to assess mood and may help diagnose depression.
Imaging
General
Memory is not the only complication of alzheimers. As the disease progresses behavioural and psychological symptoms of dementia, including sleep inversion, incontinence, excessive inappropriate motor activity (eg pacing), shouting and agitation manifests and all need individual treatment.
Medical treatment
Cholinesterase inhibitors improve alertness and function and can maintain cognitive scores at or above the baseline for up to 12 months. However, they do not modify the underlying progression of pathology.
Cholinesterase inhibitors (Donepezil) inhibit the enzyme that normally breaks down Ach →↑Ach activity. In Alzheimer’s there is ↓Ach. Side effects: particularly anorexia, nausea and vomiting. Other adverse effects include diarrhoea, insomnia, vivid dreams, cramps, dizziness, depression, lethargy, fatigue, drowsiness, tremor, weight loss, urinary incontinence and sweating.












Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion