Anal Fissure


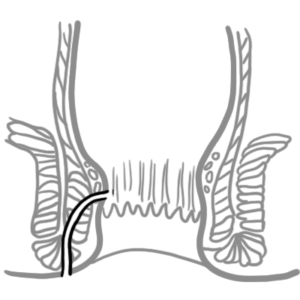
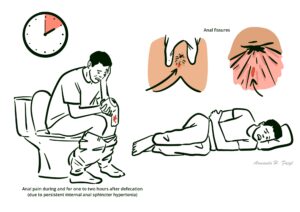
Anal fissure is a split in the skin of the distal anal canal. It presents with severe pain on defecation, like passing “glass shards”, and rectal bleeding. It is more frequently diagnosed in younger and middle-aged individuals. Anal fissures are mostly caused by passage of hard stool but can also be a result of other conditions, like Crohn’s disease.1,2
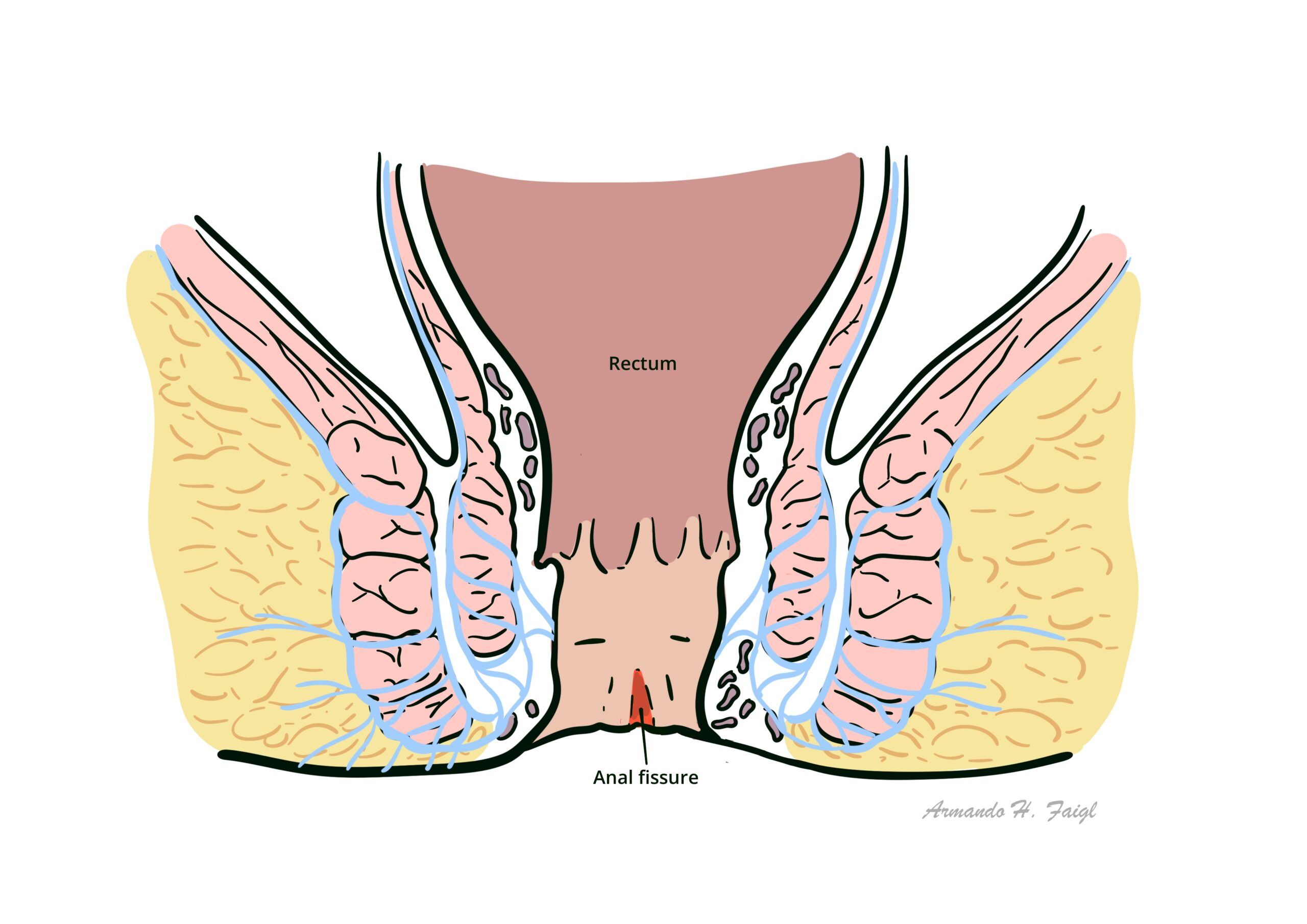
Anal fissure: linear tear within the anal canal that usually extends from the dentate line toward the anal verge.
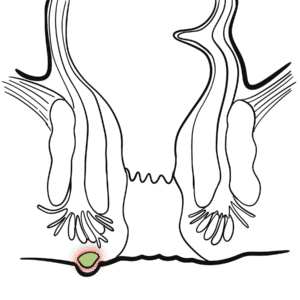
Fistula in ano: abnormal communication between anorectal lining and perineal or vaginal epithelium; nearly always associated with anal abscess.
Perianal abscess: abscess within soft tissue surrounding the anal canal.
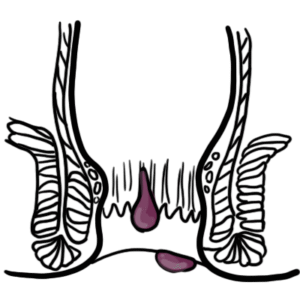
Anal haemorrhoids: dilation of either the internal or external haemorrhoidal plexi.
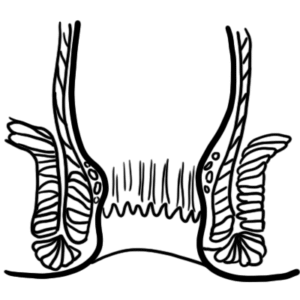
Anal canal – channel connecting the rectum to the anus, located within the anal triangle of the perineum, between the two ischioanal fossae.
Anal Sphincters
Intersphincteric plane
Anal glands
Dentate (pectinate) line
| Above Dentate line | Below Dentate line | |
| Embryology | Hindgut (endoderm) | Proctodeum (ectoderm) |
| Epithelium | Columnar | Stratified squamous |
| Arterial supply | Superior rectal a. | Middle rectal a.Inferior rectal a. |
| Venous drainage | Superior rectal v. | Middle rectal v.Inferior rectal v. |
| Nerve supply | Visceral – Inferior hypogastric plexus(insensitive to pain) | Somatic – Inferior rectal nerves: branches of Pudendal nerve(sensitive to pain) |
Hilton’s Line also called while line/anocutaneous line indicates lower end of the internal sphincter. Ischiorectal abscess when communicates with anal canal usually opens at or below Hilton’s line.
Acute trauma or another disease
↓
Internal anal sphincter spasm
↓
Local ischaemia
↓
Impaired healing
↓
Hard stool passage causing a skin tear that cannot heal
Based on aetiology:
Based on timeframe:
General inspection
Palpation: to reproduce anal pain if fissure cannot be visualised – performed to confirm diagnosis.
Digital rectal exam and anoscopy are not recommended during initial presentation due to associated pain; can be performed after symptoms have improved.
Not usually indicated, unless diagnosis is uncertain or secondary fissure suspected
Medical management:
Surgical management:
Lateral internal sphincterotomy is the gold standard unless there is high risk of incontinence.
Complication
Prognosis
1. Paluvoi N. Anal fissure: BMJ Best Practice; 2023 [updated 2023 Dec 22; cited 2025 Sep 28]. Available from: https://bestpractice.bmj.com/topics/en-gb/563.
2. Gerbasi L, Ashurst JV. Anal Fissures: National Library of Medicine; 2025 [updated 2025 Sep 15; cited 2025 Sep 28]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526063/.
3. Davids JS, Hawkins AT, Bhama AR, Feinberg AE, Grieco MJ, Lightner AL, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anal Fissures. Disease of the Colon & Rectum. 2022;66(2):190-9. Doi: 10.1097/DCR.0000000000002664
4. Madalinski MH. Identifying the best therapy for chronic anal fissure. World Journal of Gastrointestinal Pharmacology and Therapeutics. 2011;2(2):9-16. Doi: 10.4292/wjgpt.v2.i2.9
5. Bleday R. Anal fissure: Medical management. Up To Date [updated 2023 May 19; cited 2025 Sep 28]. Available from: https://www.uptodate.com/contents/anal-fissure-medical-management.
6. Stewart DB. Anal fissure: Clinical manifestations, diagnosis, prevention. Up To Date [updated 2025 Mar 19; cited 2025 Sep 28]. Available from: https://www.uptodate.com/contents/anal-fissure-clinical-manifestations-diagnosis-prevention.









Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.


Discussion