Paediatric Orthopaedics Overview

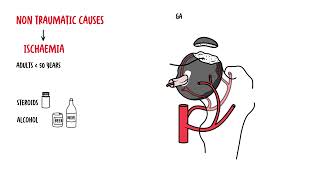
Osteochondroses is a condition that affects the epiphysis of bones. Pathology consists of localised area of ischaemic bone necrosis and oedema of adjacent soft tissue.
Osteochondroses result in avascular necrosis of the epiphyseal bone, similar to Perthes disease, but less common. In general osteochondroses is more troublesome than serious.
Age effects usually 10-15 +/-
Clinical Feature Ache and muscle spasm +/- pain
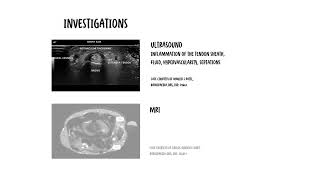
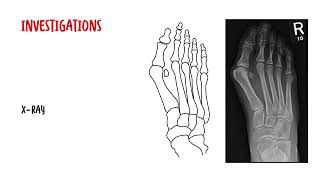
Diagnosis Clinical + X-ray
Management Usually self-resolving (except slipped capital femoral epiphysis). Manage with streatching and NSAIDs
| TYPES OF OSTEOCONDRITIDES | ||
| Osteochonroses | Features | Treatment |
| Scheuermann’s Condition | Increased kyphoses and mid/low thoracic back pain | Observe, reassurance, encourage exercise and standing straight. Physiotherapy can help. |
| Chondromalacia patellae | Pain in the knee or distal thigh and a limp | Resolves within 1-2 years. Quadricep stretch recommended |
| Osgood Sclatter condition | Pain and swelling over tibial tuberosity exacerbated by jumping or diret pressure (kneeling) | Resolves within 1-1.5 years. Quadricep stretch recommended |
| Sever Condition | Posterior heel pain with activity and shoe wear | Resolves 1 year. Calf stretch recommended |
| Normal development |
| Varus (birth-24 months) |
| Neutral (18-24 months) |
| Valgus (4-7 years) |
| Neutral/Slight Vulgus (7- adults) |
| Knock Knees (Venu Valrum) | Bow Legs (Genu Varum) | |
| Feature | Angular deformity at the knee where the apex of the deformity points toward the midline | Angular deformity at the knee where the apex of the deformity points away from the midline |
| Physiologic normal | Between ages 2-7 yo | <2 y0 |
| Investigate | <2years or >7years. Unilateral an/or symptomatic | > 2 years. Unilateral, gait abnormalities |
| Pathological | Fractures especially physeal fractures, rickets, skeletal dysplasia, neoplasms | Blount disease (cartilage disorder), rickets, skeletal dysplasia, trauma, infection, neoplasm |
| Treatment | Surgery usually required or treatment for systemic conditions | Surgery usually required or treatment for systemic conditions |
Overview
Hip pain and problems are common in children and are caused by a variety of things. Children may present with knee pain, but actually hip problem in origin. This is due to referred pain from the hip to the knee, which is common.
| COMMON CAUES OF HIP PAIN IN CHILDREN | ||
| Condition | Features | Treatment |
| Transient synovitis of the hip | Cheif cause of hip pain in children. It is usually diagnosed by exclusion. | Observation, rest and analgesia |
| Perthes’ disesae | 3-11 yo. Osteochondritis of the femoral head, secondary to avascular necrosis of the developing femoral head. More common in males (4:1), bilateral 15%. | Monitor, early arthritis. Surgery is inevitable |
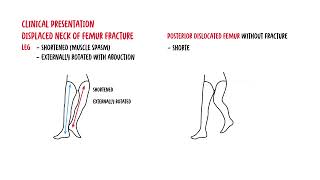
| Slipped capital femoral epiphysis | 10-16 yo. Limp, usually in an overweight child (50%), commonly in males (3:1), bilateral 20%. The affected limb will be shorter and lies in external rotation. abduction is limited when hip is flexed and internally rotated | Surgery with screw fixation across the physis to prevent furtehr slip |
| Tubercular arthritis | 2-5yo and the elderly. Rare condition. All hip movements cause pain and hip spasm | Rest. Anti-tuberculosis drugs. +/- Arthrodesis |
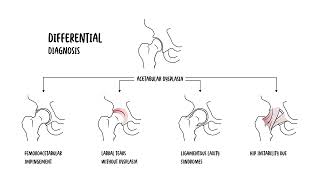
Developmental Hip Dysplasia
More info on Congenital Hip Dysplasia
Scoliosis: lateral curvature of the spine (>10º of curvature). Typically accompanied by a degree of spinal column rotation.
Idiopathic scoliosis: scoliosis with no definite etiology unlike neuromuscular, congenital, or syndromic types.
Overview 80-85% of cases occur in adolescents (children over 10 years of age)
PA standing spine radiograph
Management depends on degree of severity
More to come
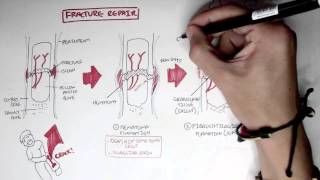
Rules of 2’s for fracture: 2 views: AP and lateral, 2 joints: above and below- exclude dislocation, 2 times: ensure fracture not shifted after 1 week, 2 sides: contralateral side for comparison.






Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.


Discussion