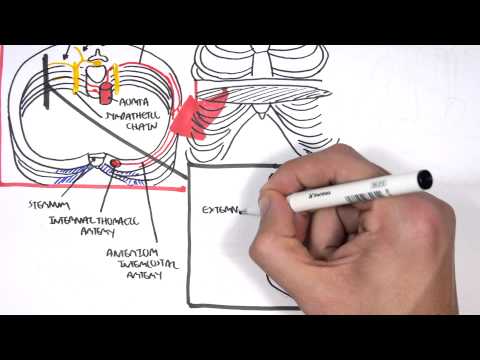
0:00 Laryngeal nerve palsy usually refers to the palsy of the recurrent laryngeal 0:11 nerve. 0:11 The recurrent laryngeal nerve is responsible for both abduction, opening, and 0:18 adduction, 0:19 closing of the vocal cord. 0:22 Therefore, recurrent laryngeal nerve palsy is also called vocal cord paralysis, 0:28 and may 0:28 be the first presentation of severe pathology such as cancer. 0:32 People often present with hoarseness, coughing, and exertional dyspnea. 0:37 In this video, we will focus on the laryngeal nerves. 0:41 Understanding the anatomy of the laryngeal nerve is important in understanding 0:45 the pathologies 0:45 that may arise. 0:47 The vagus nerve runs a complex course. 0:50 The vagus nerve exits the brainstem and descends and supplies, innovates many 0:55 organs, including 0:56 the heart, lungs, and gastrointestinal tract. 1:00 The right and left vagus nerve descends along the trachea behind the common car 1:06 otid artery. 1:07 As the vagus nerve descends down, it gives off a few branches. 1:12 The superior laryngeal nerve, which branches into the external and internal l 1:17 aryngeal nerves. 1:20 The external laryngeal nerve supplies the crack with thyroid muscle, the tuning 1:25 fork 1:25 of the larynx, responsible for raising pitch. 1:29 The internal laryngeal nerve is responsible for sensation of the larynx above 1:35 the vocal 1:35 cords. 1:38 The right vagus nerve tracks down and gives off another branch called the right 1:43 recurrent 1:44 laryngeal nerve, which loops under the right subclavian artery, turning back in 1:49 a catholic 1:49 direction to run in the tracheo esophageal group. 1:55 Similarly, the left vagus nerve descends and gives off another branch, the left 2:01 recurrent 2:02 laryngeal nerve, which loops under the aortic arch, turning back in a catholic 2:11 direction. 2:12 The right and left recurrent laryngeal nerve supplies all the muscles of the l 2:17 arynx except 2:18 the crack with thyroid muscle, which is supplied by the external branch of the 2:23 superior laryngeal 2:24 nerve. 2:25 The recurrent laryngeal nerve is responsible for the abduction, the opening and 2:31 the adduction 2:32 closing of the vocal cords. 2:36 The left and right recurrent laryngeal nerve is also responsible for sensation 2:40 of the larynx 2:41 below the vocal cords. 2:44 Additional motor function of the lower pharynx and upper esophagus is supplied 2:48 by direct 2:49 pharyngeal branches of the vagus and recurrent laryngeal nerve. 2:53 Knowing the anatomy of the laryngeal nerve, we can now appreciate that if the 2:59 recurrent 3:00 laryngeal nerve or the superior laryngeal nerve is injured, people can develop 3:04 hoarseness 3:05 of the voice. 3:07 The reason is because the superior and recurrent laryngeal nerve supply the 3:11 intrinsic muscles 3:12 of the larynx, important in vocal cord movement. 3:15 Further, when injured, the nerves will affect sensation below or above the 3:22 vocal cords. 3:23 The left laryngeal nerve is likely to be paralyzed twice as frequently as the 3:28 right. 3:29 Because of its close proximity or relationship to many intrathoracic structures 3:35 , remember 3:36 the left recurrent laryngeal nerve is the one that loops under the aortic arch 3:41 and so 3:41 it's close to the heart and the lungs. 3:45 But the pathophysiology of the laryngeal nerve palsy is a bit more complicated. 3:52 Let's focus on recurrent laryngeal nerve palsy specifically now. 3:59 Here we are looking at a person who is about to be intubated. 4:03 Now, this is the view of the vocal folds we will be focusing on. 4:09 Under normal circumstances, the vocal cords meet in the midline during phon 4:16 ation. 4:17 On inspiration, they move away from each other. 4:21 They return toward the midline on expiration, leaving a small opening between 4:27 them. 4:27 Remember, the recurrent laryngeal nerve is responsible for abduction, opening 4:34 and adduction 4:35 closing of the vocal cords. 4:38 So technically, it opens the vocal cords during inspiration, abduction, and 4:45 closes them during 4:46 phonation and expiration, adduction. 4:51 The abductor fibers, the opening fibers, are more vulnerable and moderate 4:56 trauma causes 4:57 a pure abductor paralysis. 5:00 Severe trauma causes both abductor and adductor fibers to be affected. 5:05 Therefore, recurrent laryngeal nerve palsy can be incomplete, affecting only 5:11 the abductor, 5:12 the opening fibers, or complete, affecting both abductor and adductor fibers, 5:20 the opening 5:20 and closing fibers. 5:23 Recurrent laryngeal nerve palsy can also be unilateral or bilateral, affecting 5:28 one side 5:28 or affecting both vocal cords. 5:32 Incomplete unilateral palsy, which means really unilateral abductor palsy, both 5:39 cords meet 5:40 in midline on phonation, because the adductors, the closing fibers, closes the 5:47 vocal cords, 5:48 and it's still possible on the affected side. 5:52 However, only the normal cord abducts, opens during inspiration. 5:58 For example, here is unilateral right abductor palsy. 6:04 The right vocal cord does not open with inspiration, because the right 6:08 recurrent laryngeal nerve 6:10 is injured. 6:12 However, on phonation, the adductor works, so the vocal cords can close, even 6:19 on the affected 6:20 side. 6:23 In the case of complete unilateral palsy of the recurrent laryngeal nerve, both 6:30 abductor 6:31 and adductor are affected. 6:34 On phonation, the normal unaffected cord crosses the midline to meet its 6:40 paralyzed counterpart, 6:42 appearing to lie in front of the affected cord. 6:45 For example, here, the left side is normal, and on phonation, it crosses mid 6:51 line to the 6:52 completely paralyzed right vocal cord. 6:56 On inspiration, the unaffected cord moves to full abduction, whereas the 7:05 affected right 7:07 vocal cord is unable to open and is unable to meet midline due to loss of the 7:14 closing 7:15 fibers as well, the adductors. 7:19 Incomplete bilateral palsy, which means damage to abductor fibers bilaterally, 7:28 here the adductors, 7:30 the closing fibers, draw the cords towards each other. 7:35 During inspiration, abduction, opening does not occur, and the cords, the vocal 7:42 cords, 7:43 do not open. 7:44 In you cannot open your vocal cords during inspiration, this results in severe 7:49 respiratory 7:50 distress. 7:52 Again, during phonation, the vocal cords stay closed. 7:58 On the other hand, with a complete bilateral palsy, both the abductors and ad 8:05 ductor fibers 8:06 are affected on both sides, this means that the adductor fibers do not close 8:14 the vocal 8:15 cords fully, because they're unable to. 8:18 And on inspiration, the vocal cords sort of open, a reasonable glottic opening 8:26 exists. 8:27 On phonation again, the vocal cords do not close properly, because of bilateral 8:35 loss 8:35 of adductors, the closing fibers. 8:39 Thus, bilateral incomplete palsy is more dangerous than bilateral complete pals 8:50 y. 8:50 Damage to the external branch of the superior laryngeal nerve, or to the 8:55 superior laryngeal 8:57 nerve trunk, causes paralysis of the cricothyroid muscle, the tuning fork of 9:02 the larynge, resulting 9:03 in hoarseness that improves with time, because of increased compensatory action 9:08 of the opposite 9:09 muscle. 9:11 When someone presents with hoarseness, it's important to think about injury to 9:14 the laryngeal 9:15 nerves. 9:16 However, it's important to take a step back and remember other differential 9:19 diagnoses 9:20 of hoarseness, which can be divided into organic or functional causes. 9:26 Functional causes include overuse or abuse of the voice. 9:31 Organic causes of hoarseness are things such as cancer invading the laryngeal 9:37 nerves. 9:38 A good proportion of laryngeal nerve palsy is due to cancer, which can be of 9:42 the thyroid, 9:43 esophagus, the bronchus, or hypopharynx, and these can cause compression of the 9:50 laryngeal 9:51 nerve, causing hoarseness. 9:54 Another cause is eatrogenic injury to the laryngeal nerve during surgery. 10:00 Laryngeal nerve palsy is not uncommon after operations, including thyroidectin 10:06 ies, parathyroid 10:08 ectinies, esophageal and parengeal surgery. 10:12 Again, these operations are performed in very close proximity to the laryngeal 10:18 nerve. 10:19 Other causes include neck trauma from any cause such as motor vehicle accident 10:24 resulting 10:24 in laryngeal nerve injury, degenerative neural disorder such as motor neuron 10:29 disease and 10:30 demyelinating disease such as multiple sclerosis. 10:33 Another cause are brain stem strokes as well as cerebral strokes. 10:39 Bilateral vocal cord paralysis is usually a result of eatrogenic things 10:46 secondary to 10:47 neck surgery or tracheal intubation, which may accidentally compress the laryn 10:54 geal nerve. 10:55 Bilateral vocal cord paralysis either incomplete or complete is also seen in 11:00 many neurological 11:01 disorders such as motor neuron disease, diabetic neuropathy, myasthenia gravis, 11:07 and strokes. 11:10 I hope you enjoyed this video on laryngeal nerve palsy, thank you for watching.