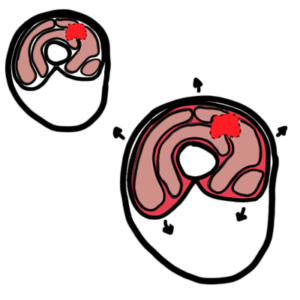
0:00 A subarachnoid hemorrhage is a type of stroke that causes bleeding around the 0:09 brain. 0:10 Subarachnoid hemorrhage, the bleeding, happens in part of the head called the 0:13 subarachnoid 0:14 space. 0:16 This is the area between the arachnoid and pia matter, which is the meninges of 0:20 the brain, 0:21 a layer that protects the actual brain. 0:24 Normally you have cerebrospinal fluid floating around the subarachnoid space. 0:29 But with a subarachnoid hemorrhage, you see blood occupying this area. 0:38 Most spontaneous subarachnoid hemorrhages are caused by ruptured, secular aneur 0:44 ysms. 0:44 If the secular aneurysm is large enough, it actually weakens the walls of the 0:48 blood vessel 0:50 causing rupture and hemorrhage. 0:53 Other types of aneurysms can also include fusiform aneurysm and mycotic aneurys 0:59 ms, secondary 0:59 to infectious organism. 1:02 Other causes of subarachnoid hemorrhage, side-terminal aneurysm include occult 1:08 trauma, atrovenous 1:09 malformations or fistula, vasculidities, intracranial arterial dissection, amyl 1:16 oid 1:16 angiopathy, bleeding diathesis and illicit drug use, especially the use of 1:22 sympathomimetics 1:23 such as cocaine and amphetamines. 1:26 We will focus on the most common cause of subarachnoid hemorrhage, which is 1:30 from an aneurysm. 1:32 But all the pathophysiology that follows can be related back to any of the 1:38 causes. 1:38 Now specifically for the aneurysm, the risk of an aneurysmal rupture includes 1:44 the size 1:45 of the aneurysm, how quickly it grows, the site of where the aneurysm is. 1:50 So for example, posterior circulation aneurysm involving the vertebral basilar 1:56 artery or the 1:57 posterior communicating arteries have the highest rates of rupture. 2:03 Physical exertion is a risk, hypertension, smoking, alcohol, and the use of 2:09 sympathomimetics. 2:11 When an aneurysm ruptures, bleeding occurs in the subarachnoid space, causing 2:17 subarachnoid 2:18 hemorrhage. 2:20 Note that with a ruptured aneurysm, there can also be a concurrent intercere 2:27 bral hemorrhage 2:29 as well as an intraventricular hemorrhage bleeding within the ventricles of the 2:36 brain. 2:37 The classic clinical presentation is a sudden onset, severe headache, worst 2:43 headache ever. 2:44 Some people also describe it as a blow to the back of the head. 2:50 They may also describe what's called a sentinel headache, which is a severe 2:54 headache preceding 2:56 the actual rupturing of the aneurysm. 3:00 Patients may also have neck stiffness, vomit, and have an altered level of 3:04 consciousness 3:04 or loss of consciousness. 3:10 Examination findings include hypertension, meningismus, neck stiffness, and 3:16 photophobia, 3:17 medicine syndrome, which is where if you look at the back of the eye, you can 3:22 see multiple 3:23 vitrous hemorrhage. 3:26 They may have signs of raised intracranial pressure and/or any new neurological 3:32 deficit. 3:33 For example, a third nerve palsy is associated with a posterior communicating 3:40 artery aneurysm. 3:42 Subarachnoid hemorrhage is a medical emergency because it can cause death. 3:46 In the first 24 hours, re-bleeding from the site of the aneurysmal rupture can 3:52 occur. 3:52 This occurs in up to 15% of people and is associated with high mortality. 3:57 Re-bleeding is characterized by any new neurological deficit. 4:02 Subarachnoid hemorrhage can lead to hydrocephalus, which can be an early or 4:06 late complication, 4:08 occurring in about a quarter of the patients. 4:12 What happens here is that you have an obstruction of the cerebrospinal fluid 4:18 flow because of 4:19 the blood products in the subarachnoid space. 4:23 As a result, there is reduced cerebrospinal fluid absorption at the arachnoid 4:30 granulation. 4:31 Cerebrospinal fluid accumulates within the subarachnoid space, leading to what 4:35 is known 4:35 as hydrocephalus. 4:38 Other immediate complications include intracerebral hemorrhage, and depending 4:43 on the hemorrhage 4:44 volume, this can lead to significant increase in intracranial pressure. 4:49 An increase in intracranial pressure means the pressure is elevated inside the 4:55 cranium, 4:55 the skull head. 4:57 When the pressure inside your skull and around your brain increases, you can 5:01 imagine it would 5:02 cause a lot more complications. 5:06 An increase in intracranial pressure leads to early brain injury due to reduced 5:12 cerebral 5:12 blood flow, reduced blood flow to the brain, and this will cause what is called 5:18 transient 5:18 global cerebral ischemia. 5:24 To appreciate the mechanism behind this, you need to appreciate that normally 5:28 blood vessels 5:29 supplying the brain are "patent" and allow oxygenation of tissues easily. 5:36 With subarachnoid hemorrhage, there are pathological changes as a response to 5:41 the injury, bleeding 5:42 and inflammation. 5:44 This includes vasoconstriction, microthrombus formation, endothelial damage of 5:49 the surrounding 5:50 cells, apoptosis of the cells, and cerebral edema. 5:56 From extravasation, the movement of fluid from the blood vessel out to the 6:01 brain tissue. 6:03 All in all, what happens is that you get reduced blood flow as a response 6:09 leading to early 6:10 brain injury. 6:17 Over time, an increase in intracranial pressure causes death due to reduced 6:21 cerebral blood 6:22 flow and acute cardiopulmonary changes. 6:27 Another common complication of subarachnoid hemorrhage is vasospasm, which 6:31 occurs 3-14 6:32 days after the injury. 6:34 Vasospasm is where the blood vessels in the brain spasm, causing altered 6:38 neurological 6:39 status every time this happens. 6:42 Vasospasm is thought to be a result of lysis of subarachnoid blood and damage 6:48 endothelial 6:48 cells, causing reduced nitric oxide production and increased endothelial 6:54 production, causing 6:55 the vasoconstriction that we see. 6:58 Vasospasm in turn can cause delayed cerebral ischemia and infarction. 7:04 Delayed cerebral ischemia occurs in approximately 30% of patients with aneurys 7:09 mal subarachnoid 7:10 hemorrhage. 7:13 The definition of delayed cerebral ischemia requires the occurrence of a focal 7:18 neurological 7:18 impairment or a decrease of at least two points of the Glasgow Coma Scale that 7:24 lasts 7:24 for at least one hour. 7:29 Delayed cerebral ischemia may result in cerebral infarction and thus 7:35 contributing to possible 7:37 death with increased mortality. 7:41 Delayed cerebral ischemia is really similar to early brain injury, however, it 7:47 's a later 7:48 event. 7:54 Hyponatrimia is another complication and develops in up to 30% of patients with 7:57 subarachnoid 7:58 hemorrhage and is probably mediated by hypothalamic injury. 8:03 The water retention that leads to hyponatrimia may result from either the 8:07 syndrome of inappropriate 8:09 secretion of anti-diarratic hormone, SIADH, or from cerebral salt wasting. 8:16 Using SIADH, excess ADH is produced which will target the kidneys and cause 8:22 inappropriate 8:23 retention of water causing hyponatrimia. 8:30 During subarachnoid hemorrhage you have an increased sympathetic response which 8:34 can lead 8:34 to cardiopulmonary complications including neurogenic pulmonary edema and 8:41 cardiac arrhythmias. 8:44 The body's response to the central sympathetic overdrive is to produce natur 8:49 itic peptide 8:50 such as brain naturitic peptide BNP. 8:54 BNP causes naturices, essentially peeing out salt from the body. 9:01 This is one of the potential causes of hyponatrimia termed cerebral salt 9:07 wasting. 9:09 Other complications of subarachnoid hemorrhage include seizures about 15%, an 9:14 emia, hyperglycemia 9:16 which is associated with poor outcomes, fevers, it's important to differentiate 9:20 between infective 9:21 and non-infective causes of fever, and finally, hypothalamic pituitary 9:27 dysfunction. 9:29 Investigations for someone who has a subarachnoid hemorrhage or suspected is a 9:34 CT brain non-contrast, 9:36 stressed within 12 hours, and this will show blood collecting in the subarachn 9:42 oid space. 9:43 Lumbar puncture can also be performed if the CT brain is not definitive. 9:49 Lumbar puncture will show increased pressure and xantharachromia, which is the 9:53 presence 9:54 of bilirubin in the cerebrospinal fluid, secondary to the breakdown of the red 9:58 blood cells resulting 10:00 in the yellow discoloration. 10:05 It's important to maintain oxygen between 94 to 98%, if the GCS is low, intub 10:14 ation is 10:14 necessary, treat the hypertension, aim for a blood pressure less than 140mm of 10:20 systolic 10:21 pressure, anything over 150 systolic blood pressure is associated with re-ble 10:28 eding, important 10:29 to avoid hypotension as this may lead to cerebral ischemia, analgesia and anti- 10:35 medics can be 10:36 used, anti-epileptic medications may also be used to correct any coagulopathy, 10:42 so vitamin 10:42 K and prothrombin-X for warfarin, calcium channel blockers such as nebotopene 10:48 is important 10:48 to prevent secondary vasospasm, manatol intravenously is used if there is 10:54 evidence of raised intracranial 10:56 blood pressure, finally and most importantly neurosurgical review should be 11:01 done early 11:02 to secure aneurysmal bleeding through coiling or clipping if coiling is 11:10 unavailable, treat 11:12 the complications of subarachnoid hemorrhage such as hydrocephalus, either 11:16 through an 11:17 external or internal shunt or if shunt is unable to be performed right away, 11:22 intravenous 11:23 manatol can be used, in summary subarachnoid hemorrhage is bleeding within the 11:27 subarachnoid 11:28 space, the most common cause is a sacula aneurysmal rupture.