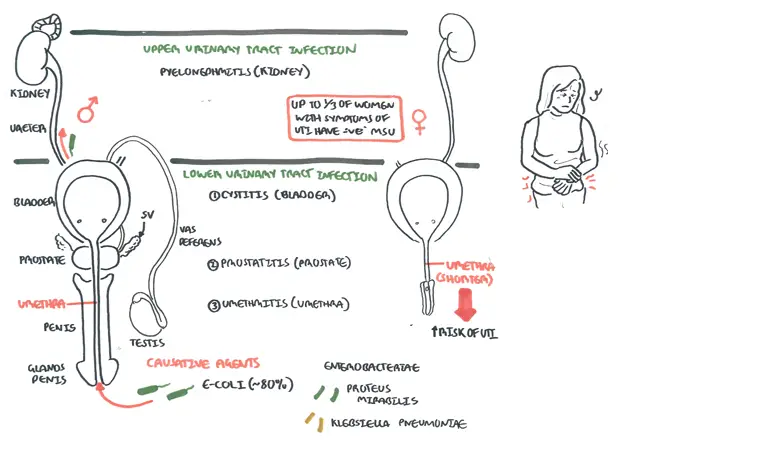
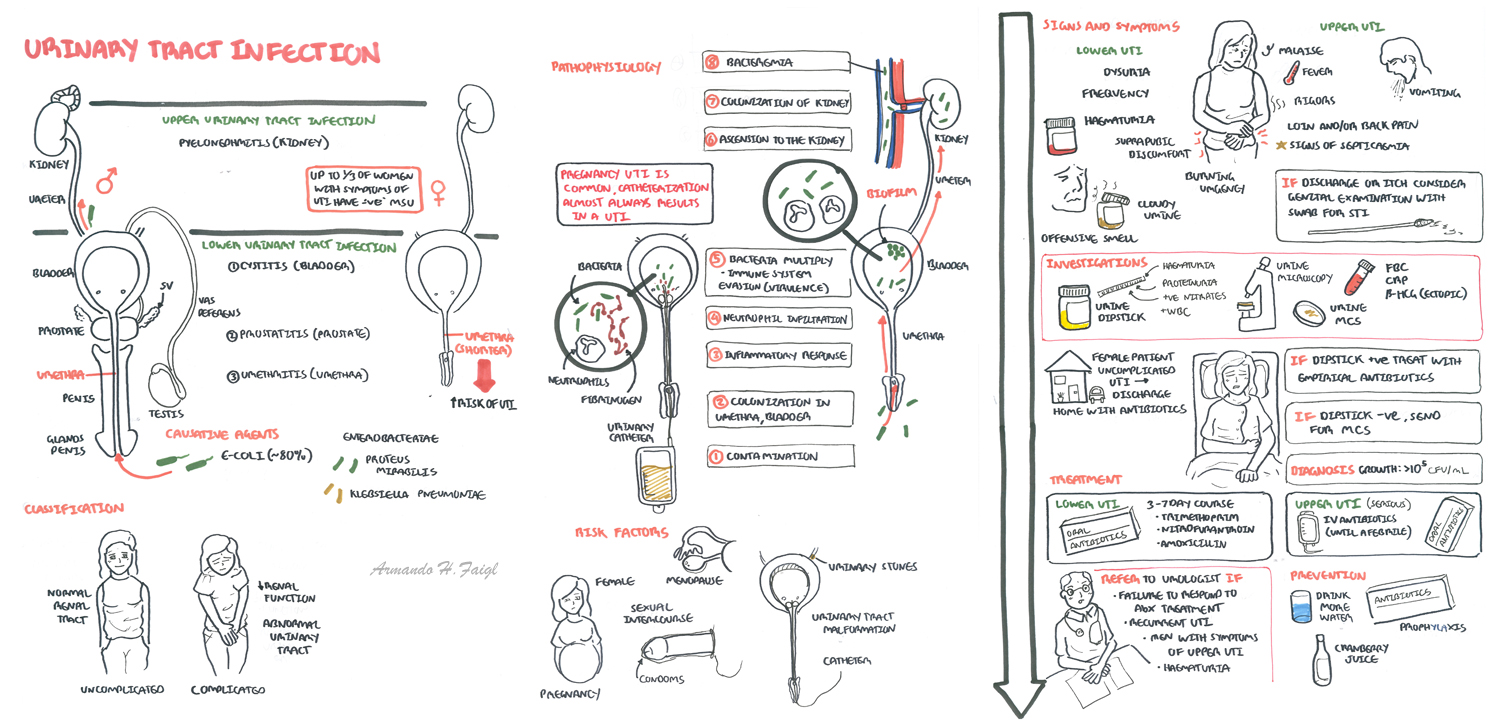
Overview Infection of the urinary tract is common and more so in women (due to shorter urethra and hormonal changes). UTIs may be classified as either a lower (Cystitis, urethritis and Prostatitis) or upper UTI (pyelonephritis). The main causative agents are bacteria such as E-coli. A lower UTI can progress to an upper UTI causing systemic symptoms and acute loin pain.
The urinary system consists of:
The kidneys are retroperitoneal bean shaped organs thats sits between veretbral levels T11-L3, the left kidney sitting slightly higher then the right kidney.
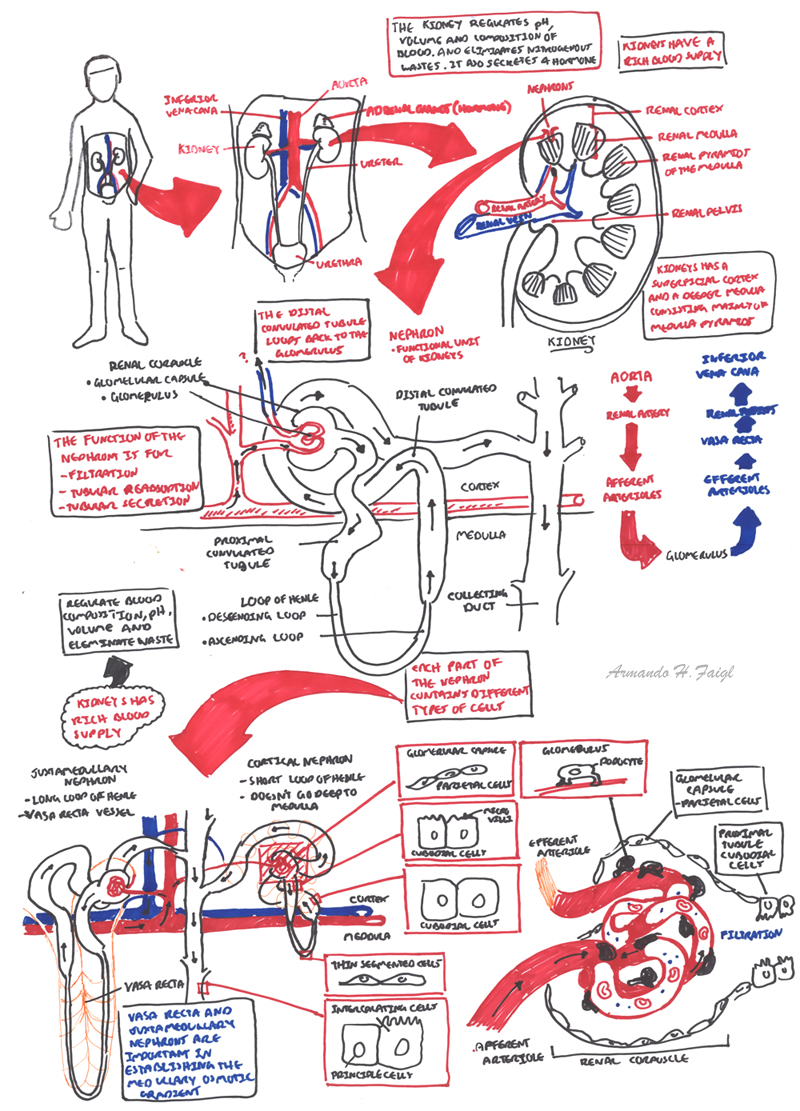
The kidneys is divided into three sections:
Arterial Supply
Venous Drainage
Nephrons
Ureters are narrow muscular tube that transport urine to the bladder. There are three narrowed areas of each ureter:
Bladder is a muscular organ which holds urine. The wall of the bladder comprises of four layers:
Urethra Arisis from the base of the bladder and is the passageway through which urine is discharged from the body. The female urethra is much shorter (3-4cm) than the male urethra (18+cm)
| Watch Video Nephrology Overview |
| Risk Factors |
| Female gender |
| Sexual Intercourse |
| Catheterisation |
| Pregnancy |
| Menopause |
| Diabetes |
| Genitourinary malformation |
| Immunosuppression |
| Urinary Tract obstruction |
Clinical Presentation - lower urinary tract infection
Clinical Presentation - upper urinary tract infection
| Side note Older people may also present with delirium, confusion, falls, immobility or anorexia |
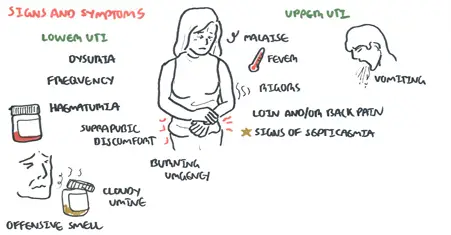
The signs and symptoms of lower and upper UTI differ
| Triad of Pyelonephritis (Upper UTI): Fever, flank/back pain and nausea/vomiting |
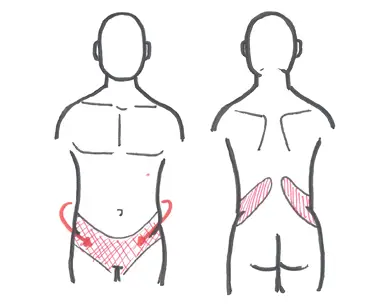
Flank/loin Pain in Pyelonephritis
Diagnosis

Pathophysiology
Lower UTI
Upper UTI

Flow chart of the management of suspected UTI. The most important investigation would be Urine analysis and bloods in the acute setting followed by empirical antibiotics
| Remember Refer to Urologist if patient fails to respond to medical treatment, has recurrent UTIs, Haemturia and men with symptoms of UTI as this is considered abnormal. |
Complications
Prognosis
| Watch video Urinary Tract Infection |