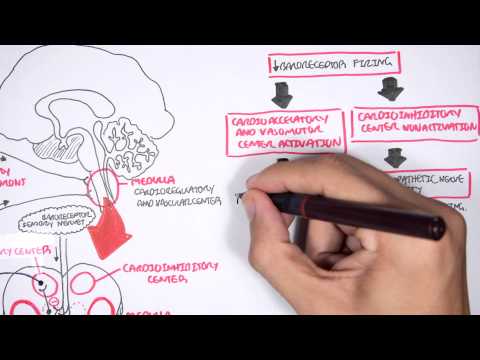
0:00 Hello, in this video we're going to talk about acute epiglottitis. 0:08 Now the epiglottis is an important structure that helps to cover the airways 0:12 during swallowing, 0:15 so that food does not enter the lungs. 0:19 Epiglottitis is inflammation of the epiglottis and the surrounding structures, 0:23 typically 0:23 by bacteria. 0:26 Epiglottitis is a life-threatening infection. 0:28 It progresses rapidly, causing profound swelling of the upper airways, which 0:32 can lead to a 0:33 fixia and respiratory arrest. 0:39 Before the introduction of the hemophilus vaccine, hemophilus influenza type B 0:43 was the 0:43 most common cause of epiglottitis. 0:46 Now group A streptococcus, a gram-positive beta hemolytic bacteria is a more 0:52 commonly 0:53 responsible agent for this infection. 0:57 Common infectious causes of epiglottitis may include trauma from foreign 1:02 objects, inhalation 1:03 and chemical burns. 1:07 The epiglottis is composed primarily of fibroelastic cartilage. 1:12 It is shaped like a leaf and is found at the base of the tongue and above the l 1:18 arynx. 1:19 The epiglottis is connected to the surrounding structures, and so during 1:23 swallowing when 1:24 the tongue-based and pharyngeal walls contract, the epiglottis will also move 1:30 and cover the 1:31 top of the airway. 1:33 This is in order to divert the food, the bolus, so that it can be swallowed 1:37 down the esophagus 1:38 rather than the trachea, the airway. 1:42 The epiglottis is close to other important structures, including the arachnoids 1:47 , ariepiglottic 1:49 folds and the volecular. 1:53 These other structures also become inflamed in epiglottitis. 2:02 In a young child, the epiglottis is located more superiorly and anteriorly than 2:07 in an 2:07 adult. 2:08 There is also a more oblique angle with the trachea. 2:12 Further, the infant's epiglottis is floppy compared to an adult, whose epiglott 2:18 is is 2:19 more rigid. 2:21 These anatomical differences are why airway compromise is much more common and 2:27 serious 2:28 in children than adults. 2:31 A bacteria can trigger an inflammatory reaction in the epiglottis, causing 2:36 immune cell infiltration 2:38 and subsequent pain, swelling, redness and erythema. 2:44 Epiglottitis occurs acutely but may be preceded by viral upper respiratory 2:51 tract infection. 2:52 In young children, the epiglottis can be visible during examination of the o 2:57 ropharynx, but in 2:58 suspected epiglottitis, the oropharynx should not be examined as it may result 3:03 in loss of 3:04 airway and cause more harm than good. 3:08 Children with epiglottitis appear toxic. 3:11 Children present with a generalized toxemia, including high fevers, severe sore 3:16 throat 3:16 and difficulty swallowing. 3:18 In spiritually strider is a later finding when the epiglottitis begins to swell 3:24 and cause 3:24 partial obstruction. 3:27 The patient may be sitting up and leaning forward in a sniffing position. 3:31 This tripod position is maintained in order to maximize the airway. 3:38 Other features include muffled voice, breathing with an open mouth and a protr 3:42 uding tongue. 3:43 The patient frequently drools because of difficulty and pain on swallowing. 3:49 Lateral neck radiograph findings can include the thumbprint sign of supraglitis 3:54 , a grossly 3:55 swollen epiglottic shadow and obliteration of the volecular known as the vole 4:01 cular sign. 4:04 There is a lateral soft tissue radiograph of the neck with the thumbprint sign 4:09 in epiglottitis, 4:11 which again is a manifestation of a dermatus and enlarged epiglottis. 4:20 Epiglottitis is a life threatening infection which can progress rapidly causing 4:25 upper 4:25 area obstruction. 4:27 If epiglottitis is suspected, it's important to get a senior doctor involved in 4:32 contact 4:32 and aesthetics and ENT doctors while waiting to sit the patient upright because 4:38 this is 4:39 the most comfortable position. 4:41 Maintain oxygen saturation by giving oxygen, cannula to take blood to send off 4:47 blood tests 4:48 and preparation for administration of intravenous antibiotics and anesthetic 4:55 agents. 4:56 An allateral radiograph can be ordered looking for signs of epiglottitis if 5:03 time permits. 5:04 Once an anaesthetist and/or ENT doctor has arrived, it's important to secure 5:10 the airway. 5:12 This can be done through airway maneuvers and nasotracheal intubation or endotr 5:17 acheal 5:18 intubation. 5:19 Crycothirodotomy kits should be present in case it needs to be used. 5:25 During intubation, the epiglottis can be visualized as cherry red. 5:30 The epiglottis is very swollen and enlarged and children have a high risk of 5:35 airway closure. 5:38 The definitive treatment is antibiotics. 5:41 Steroids are used sometimes to help reduce swelling, however, there is no 5:46 proper study 5:47 supporting this yet. 5:50 For adults, although epiglottitis is thought to be predominantly affecting 5:55 children, it 5:56 is becoming more common in adults. 5:59 For adults, superglottitis is more appropriate because inflammation tends to 6:04 affect structures 6:05 above the glottis, including the pharynx, uvula and base of the tongue. 6:11 Patients with superglottitis have predominant symptoms of odenophasia, dysphag 6:19 ia and voice 6:19 changes out of proportion to pharyngeal inflammation. 6:25 The management in adults with epiglottitis or superglottitis is the same with 6:30 airway 6:31 support and antibiotics being the most fundamental. 6:37 Applications of epiglottitis in both children and adults include airway loss 6:43 and death as 6:44 the swelling of the epiglottis and surrounding structures can cause obstruction 6:48 of the airways. 6:51 Epiglottitis is usually caused by an infection, by bacteria. 6:55 The infection can spread, for example it can cause epiglottic abscess. 7:01 It can cause descending necrotizing medius denitis, and paima as well as 7:10 pneumonia to 7:12 name a few. 7:16 I hope you enjoyed this video on acute epiglottitis, thank you for watching.