

Urinary Tract Infection (Children)

Overview
Urinary Tract infections (UTIs) in children are common and usually carry low risk. UTIs are often non-specific and can not be diagnosed on symptoms alone. A clean specimen (urine) is required for the diagnosis of UTI. Any child who is unwell, and most children under 6 months, should be admitted for IV antibiotics. The risk for child to develop a UTI in general is ~5% (girls > boys). Of these ~25% will experience recurrence within one year. However, in the first year UTI are more common in boys, uncircumcised boys are 10times more likely to develop a UTI compared with circumscribed boys.
Aetiology and Risk Factors
Aetiology
Escherichia coli (75%)
Other
- Enterococcus faecalis (~10%)
- Proteus Klebseilla
- Enterobacter
- Citrobacter
- Staphylococcus saprophyticus
- Candida albican (Fungal) – usually in immunocomprimised or following antibiotic use.
Routine Circumcision is not recommended because many (>100) boys would have to get circumcised to prevent one UTI.
Pathophysiology
UTI susceptibility is determined by:
- Bacterial virulence
- Anatomical variances
- Gender
- Vesicourethral reflux
- Circumcision
- Bowel of bladder dysfunction
- Host defences
Clinical Manifestation
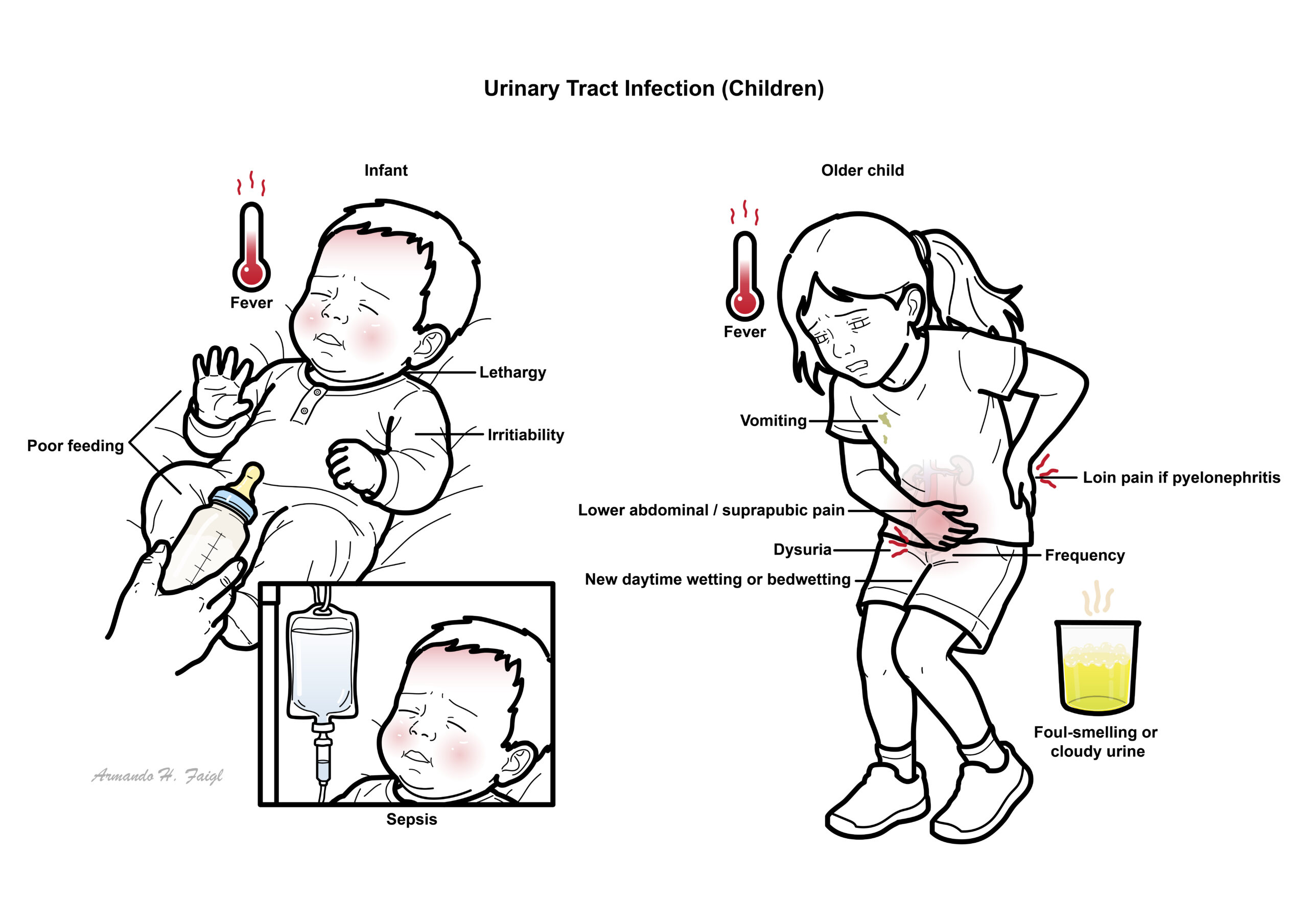
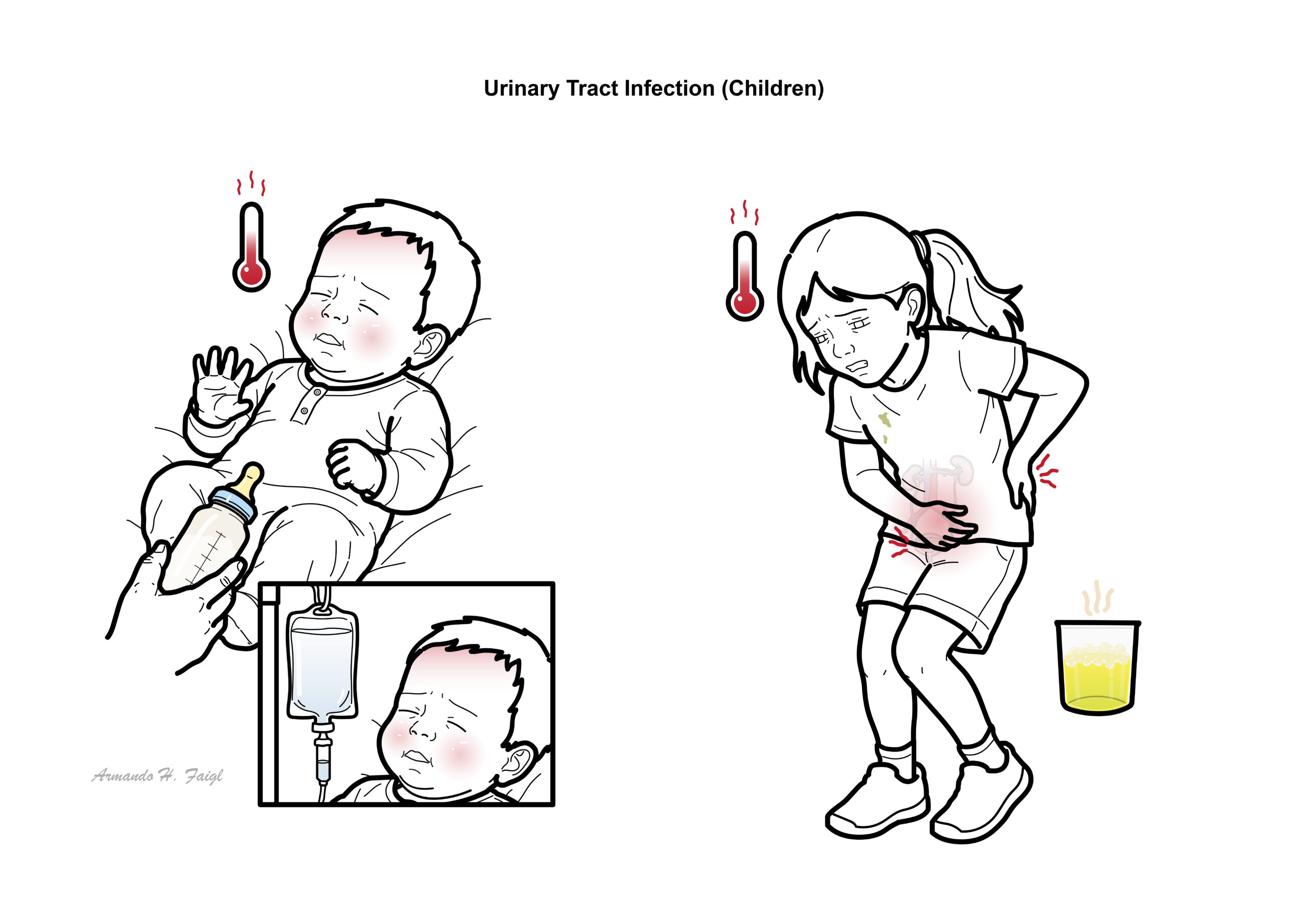
Urinary tract infection in children are often non-specific and can not be diagnosed on symptoms alone.
Infants:
Older children can present with the classic:
- Dysuria
- Frequency
- Loin Pain
Early diagnosis with appropriate urine specimen collection techniques, investigations and treatment is necessary for prevention of renal damage and recurrence.
Diagnosis
If fever and feeling unwell is the sole presenting symptom, such as seen in <2yo, think of other differentials.
- Otitis media
- Gastroenteritis
- Upper respiratory tract infection
Urine should be collected if there is a unexaplined fever and/or symptoms suggestive of UTI.
Method to obtain urine sample include:
- Bagged urine – unreliable gets contaminated, but negative sample may exclude UTI
- Clean catch
- Mid-stream
- Catheterised specimen
- Suprapubic aspiration
| Urine specimen collection methods | Advantages | Disadvantages |
| Urine bag | Non-invasiveNegative culture tests may exclude a UTI | Highest risk of contamination |
| Clean catch | Non-invasivePreferred technique for infants able to void on request | |
| Catheterisation | Presumed to be less painful and less invasive than SPA | Invasive |
| Suprapubic aspiration | Preferred asepctic methodLess likely to acquire contamination | Most invasive |
Following urine sample collection other investigations include:
- Urinalysis
Recurrent UTI investigations
- KUB ultrasound (first-line) – Assess:
- Fluid colelction
- Bladder volume
- Kidney size/shape
- Urinary Tract obstruction/dilatation
- Micturating cystourethrogram (MCU) – contrast radiographic imaging – Confirm:
- Posterior urethral valve
- Obstructive uropathies
- Diagnosing VUR
- Radoisotope nuclear imaging (DMSA and MAG3) – Confirm:
- Renal damage
A urine sample suitable for culture should be obtained before initiating antimicrobials.
Diagnosis
| Urine specimen collection methods | Diagnosis |
| Urine bag | Not suitable for diagnosis. Useful to exclude a UTI |
| Clean catch | >10^5 CFU/mL clinically releveant organisms + pyuria/bacteruria |
| Catheterisation | >10^5 CFU/mL clinically releveant organisms + pyuria/bacteruria |
| Suprapubic aspiration | Any growth of clinically relvenat organism + pyuria/bacteruria |
A diagnosis of UTI cannot be established reliably by a culture of urine collected in a bag.
Classification
- Asymptomatic Vs. Symptomatic
- Anatomically
- Single vs. Recurrent
| Recurrent UTI |
| Inadequate antimicrobial therapy |
| Non-compliance |
| Bacterial Resistance |
| Host susceptibility |
| Factors contributing to urinary stasis |
Treatment
The main aim of management is to prevent sepsis.
Non pharmacological
- Hydration
- Improve bowel habits
- Improve hygiene
Pharmacological
- IV Broad spectrum antibiotics – gentamycin + benzylpenicillen
- Switch to ceftriaxone if worried of nephrotoxicity and oxotocitiy from gentamycin
- Broad spectrum oral antibiotics (if appropriate) – Trimethoprim OR Cephalexin
- Tailor antibiotics after organisms has been cultured and antibiotic sensitivity established
Pharmacology
Gentamycin (Gentamicin) Aminoglycosides like gentamicin “irreversibly” bind to specific 30S-subunit proteins and 16S rRNA. This leads to interference with the initiation complex, misreading of mRNA so incorrect amino acids are inserted into the polypeptide leading to nonfunctional or toxic peptides and the breakup of polysomes into nonfunctional monosomes. Side effects: Nephrotoxicity and Otoxocity.
| Consider referral to paedriatic team |
| Child <6months of age |
| Child with known renal tract abnormalities |
| Any child who looked unwell and required a septic workup |
Surgical
Complications and Prognosis
- 10-30% will have recurrence within 12 months
Urinary Tract Abnormalities
Vesicoureteric reflux
- Disorder in which urine passes in a retrograde direction from the bladder through the vesicoureteric junction into the ureter
- Distal end of ureter runs less obliquely through the wall of the bladder → less muscle around it → retrograde urine flow during micturition → ureteric dilation
- Sometimes associated with renal malformation (renal scarring, dysplasia, reflux-associated nephropathy), excessive dilation & tortuosity of the ureter, and abnormalities of bladder function (premature detrusor contractions → urgency, wetting, poor bladder emptying)
- Common, affecting 40% of children <1yo who are investigated for a first UTI
- Diagnosis: MCU
- VUR often resolves spontaneously, although UTIs still often occur periodically throughout life
- Aka congenital obstructive posterior urethral membranes (COPUMs)
- Affects males, causing obstruction to urine flow at the level of the posterior urethra
- Bladder is often thick-walled & trabeculated
- There may be associated VUR with tortuous & dilated ureters draining hydronephrotic kidneys
- Presentation: antenatal USS demonstrating hydronephrosis & megacystitis is a common, as is UTI in early infancy, and some present later with dribbling & wetting
- Diagnosis: urethrogram phase of MCU + cystoscopy
- Tx: complex surgical procedures
Duplication
- Kidney has 2 separate collecting systems
- Ureters may join before entry into the bladder, or they may have separate openings
- One of the ureters may enter directly into the urethra → incontinence
- Often has VUR
Pelvicoureteric junction (puj) obstruction
- Commonly diagnosed following evaluation of hydronephrosis on antenatal scanning of the fetus
- 9/10 cases will resolve spontaneously over the first year of life
- F/U: periodic renal ultrasound DPTA or MAG3 radioisotope scans
- May present later in life with renal colic (→ usually require surgery)
- Vesicoureteric junction (VUJ) obstruction
- Presentation: often following Ix of UTI with USS showing dilated ureter & MAG3 scan showing delayed passage of urine from the ureter into the bladder
- Tx: stenting of VUJ or re-implantation of ureter
- Renal calculi
- Presentation: following UTI (usually triple phosphate calculi/stone – Mg, Ca, ammonium with Proteus infection) or renal colic
- Other stones occasionally encountered: cystine (autosomal recessive cystinuria), calcium oxalate, and uncommonly, uric acid
- Antenatal renal abnormalities: 1 in 200 infants have renal pelvis diameter (detected on 18/40 scan)
References
White, B 2011, Diagnosis and Treatment of Urinary Tract Infections in Children, American Family Physician, vol. 83, no. 4, pp. 409-415.
Royal Child Hospital Melbourne Australia Guidelines
Desai, D 2016, Paediatric urinary tract infections: Diagnosis and treatment, The Royal Australian College of General Practitioners, vol. 45, no. 8, pp. 558-564.



Members only discussions coming soon…