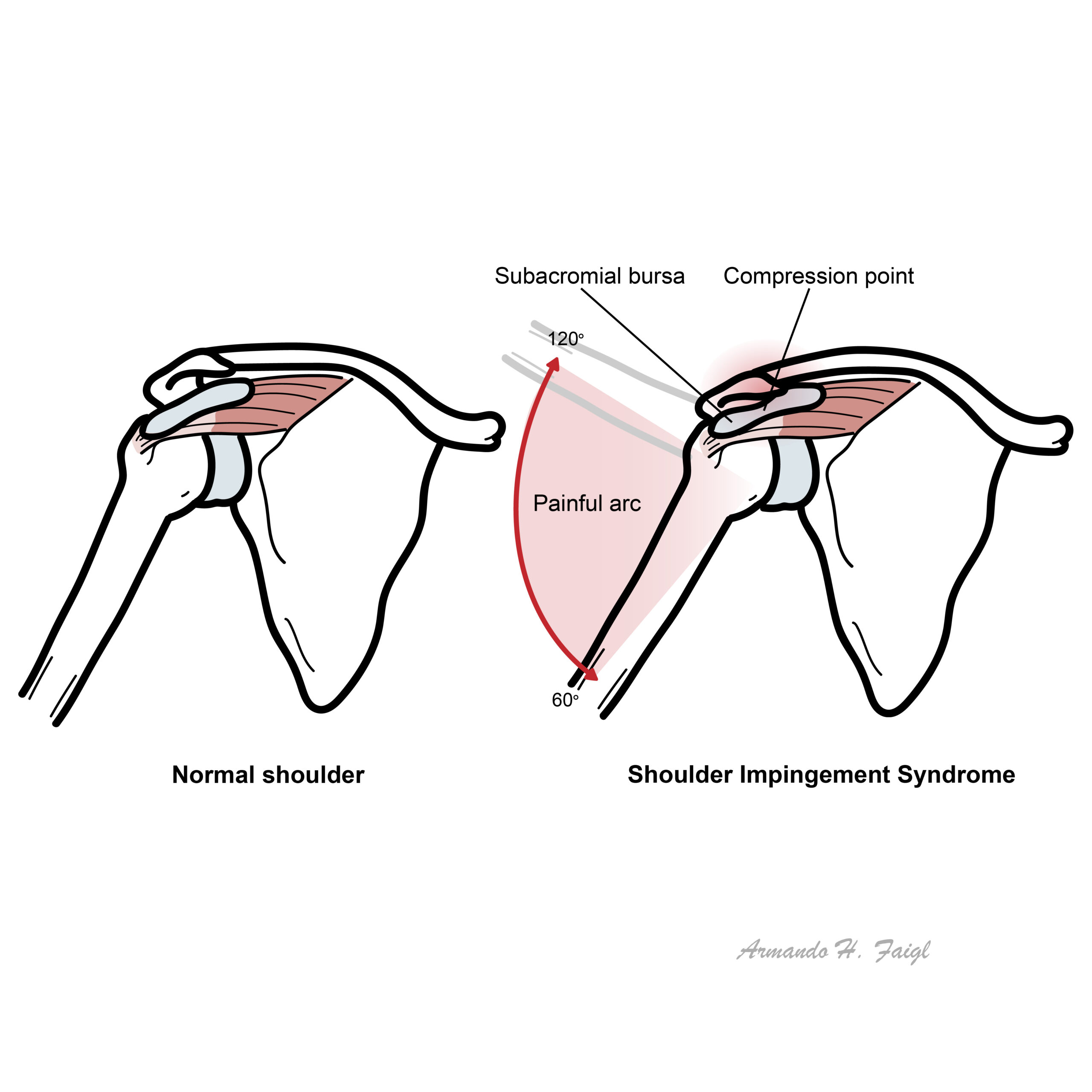
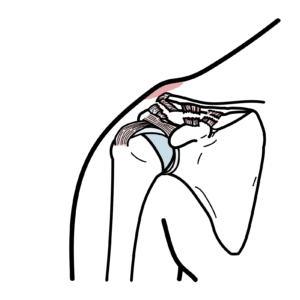
Shoulder impingement syndrome, now more commonly referred to as subacromial pain syndrome (SAPS), is one of the most frequent causes of shoulder pain. It accounts for ~40–65% of shoulder complaints in primary care and sports medicine settings. It occurs due to mechanical compression of the rotator cuff tendons (most commonly supraspinatus) and subacromial bursa beneath the coracoacromial arch, especially during arm elevation. Repetitive overhead activity, structural narrowing, or rotator cuff dysfunction all contribute.
Definition
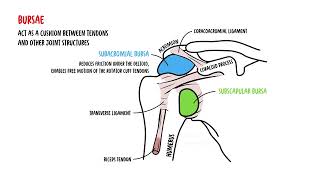
Subacromial space: Anatomical area between the humeral head and coracoacromial arch. Rotator cuff: Group of four muscles stabilising the glenohumeral joint (SITS – supraspinatus, infraspinatus, teres minor, subscapularis). Bursitis: inflammation or irritation of a bursa, which is a small, fluid-filled sac that acts as a cushion between bones, tendons, and muscles near joints. Neer sign: Pain with passive forward flexion of the arm while stabilising the scapula (suggests impingement).
Anatomy & Physiology
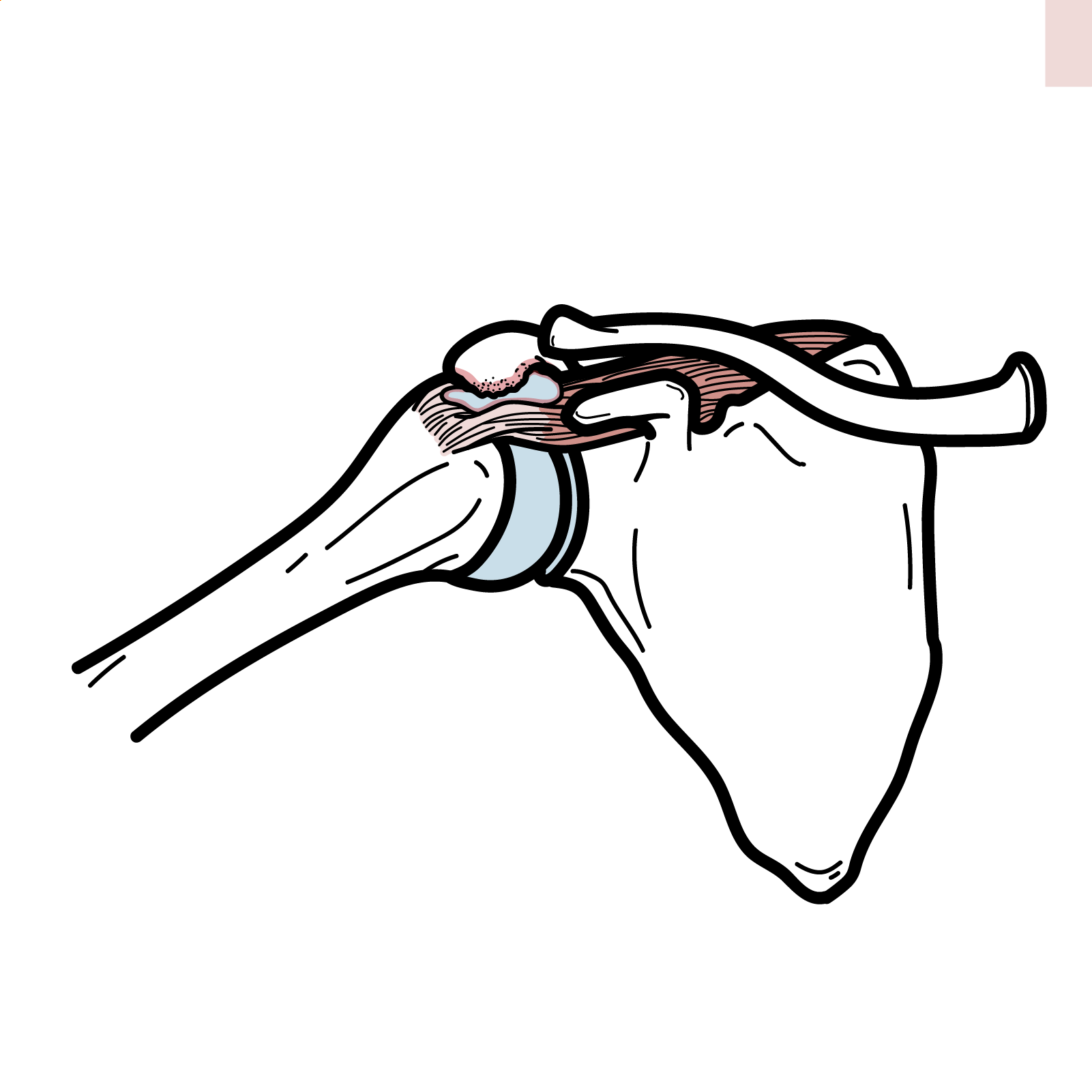
Subacromial space contents: Supraspinatus tendon, long head of biceps tendon, subacromial bursa.
Normal physiology: During abduction/flexion, humeral head depresses, allowing tendons to glide beneath acromion.
Pathology:Weakness of cuff or narrowing of subacromial space → compression/irritation → inflammation and pain.
Supraspinatus is the most commonly affected tendon.
Prognosis: Good with early management; chronic untreated cases → cuff degeneration.
Failure to treat early can convert a reversible condition into a degenerative cuff tear.
References
van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54(12):959–64.











Discussion