

Coeliac Disease
Overview
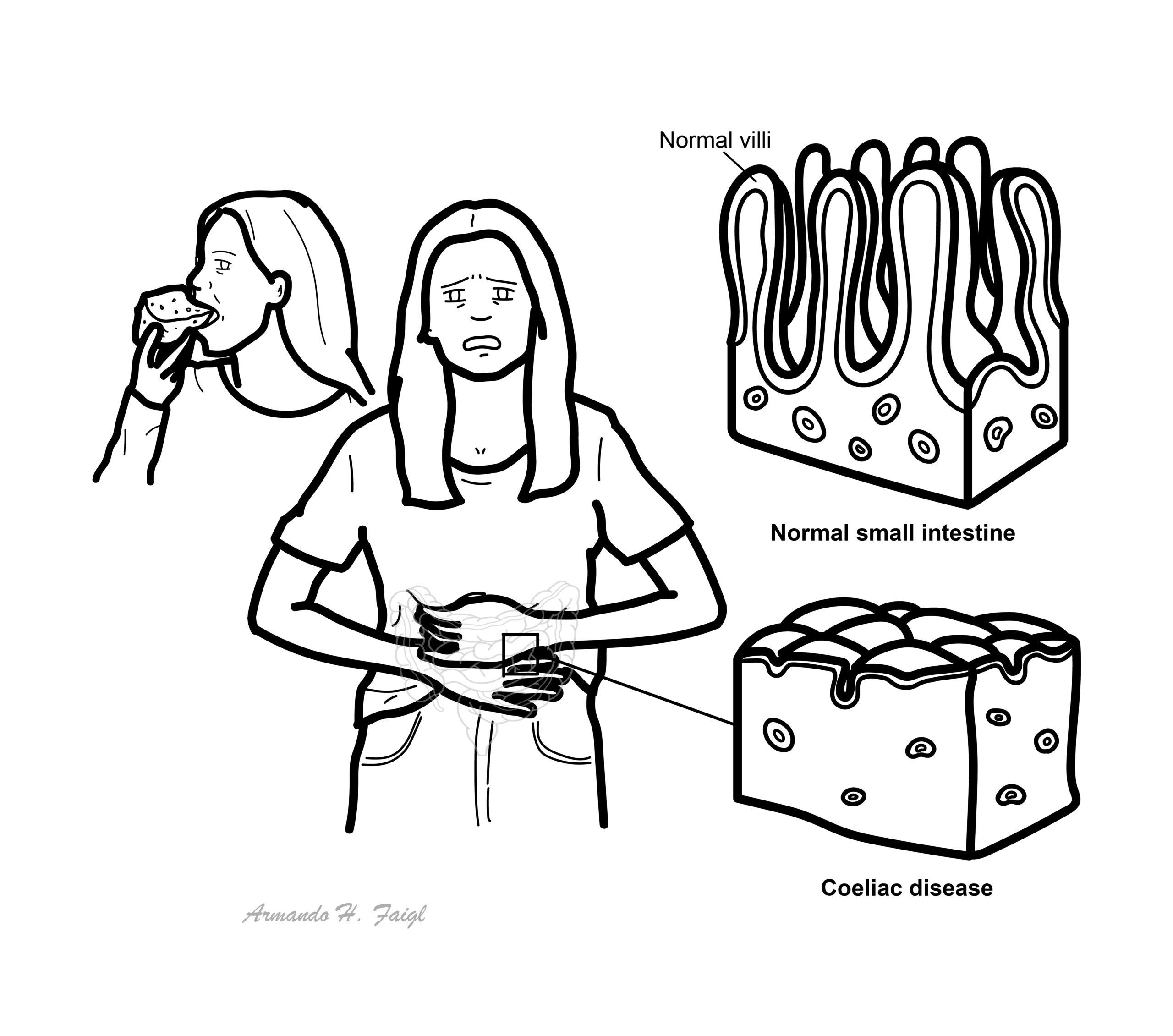
Coeliac disease is a systemic autoimmune disease triggered (T-lymphocytes) by dietary gluten peptides found in wheat, rye, barley, and related grains. Immune activation in the small intestine leads to villous atrophy, hypertrophy of the intestinal crypts, and increased numbers of lymphocytes in the epithelium and lamina propria. Locally these changes lead to gastrointestinal symptoms and malabsorption. The disease is common (1/~1000) and is more common in the Irish.
Definition
Coeliac Disease: Inflammatory process, which occurs in susceptible individuals in response to the ingestion of wheat protein (gluten and gliadin)
Gliadin: A glycoprotein (a carbohydrate plus a protein) within gluten
Anatomy and Physiology
The small intestine is divided into three sections: Duodenum, Jejunum and Ileum.
The three sections of the small intestine
- Duodenum is a secretory and digestive organ. Four parts (The second part is where the common bile and pancreatic ducts enters duodenum). The duodenum is where most of absorption takes place.
- Jejunum is a secretory and digestive organ.
- Ileum is predominantly an absorptive organ. Important in absorbing fats, vitamin B12 and IgA. The ileum is also where peyer’s patches are located which are immunological gastrointestinal sites for antigen sampling and immune cell activation.
Blood Supply (branches of the celiac trunk)
- Superior pacreaticoduodenal artery
- Posterior pacreaticoduodenal artery
Blood supply (3/5 branches of the superior mesenteric artery)
- Inferior pancreaticoduodenal artery –
- Intestinal artery
- Ileiocaecal artery (gives rise to appendiceal artery)
Physiology
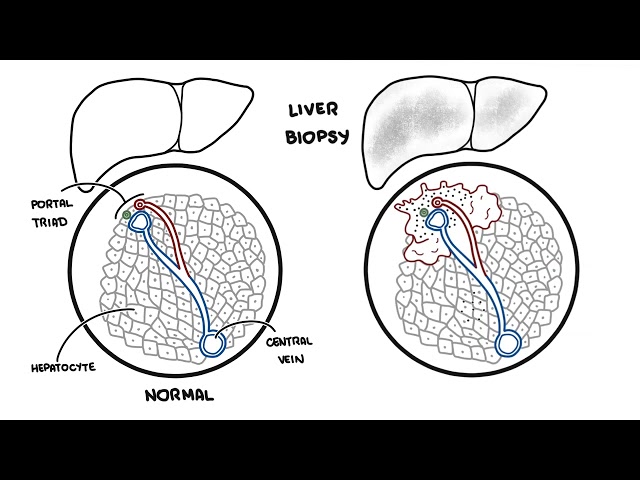
Pathophysiology
Pathology
Macroscopic
- Atrophy and scalloping of mucosal folds
- Nodular and mosaic pattern of mucosa
Microscopic
- Villous atrophy
- Hypertrophy of the intestinal crypts
- Increased numbers of lymphocytes in the epithelium and lamina propria.
Aetiology and Risk Factors
- Family history
- IgA deficiency
- Type 1 diabetes
- Autoimmune diseases – autoimmune thyroid, Sjogren’s syndrome, Addison’s disease
- Inflammatory Bowel disease
- Genetic disorder – Down’s syndrome, Turners syndrome
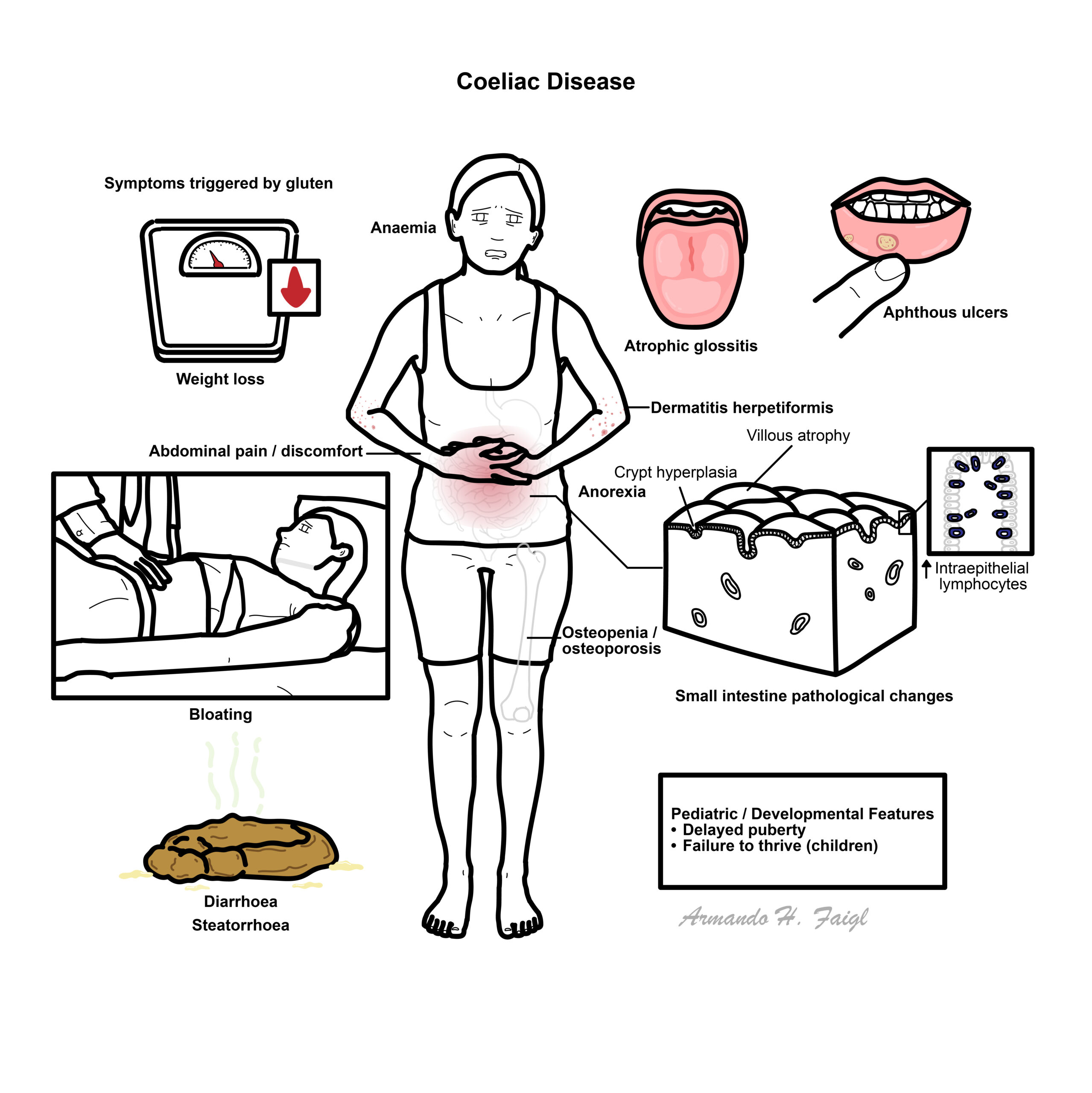
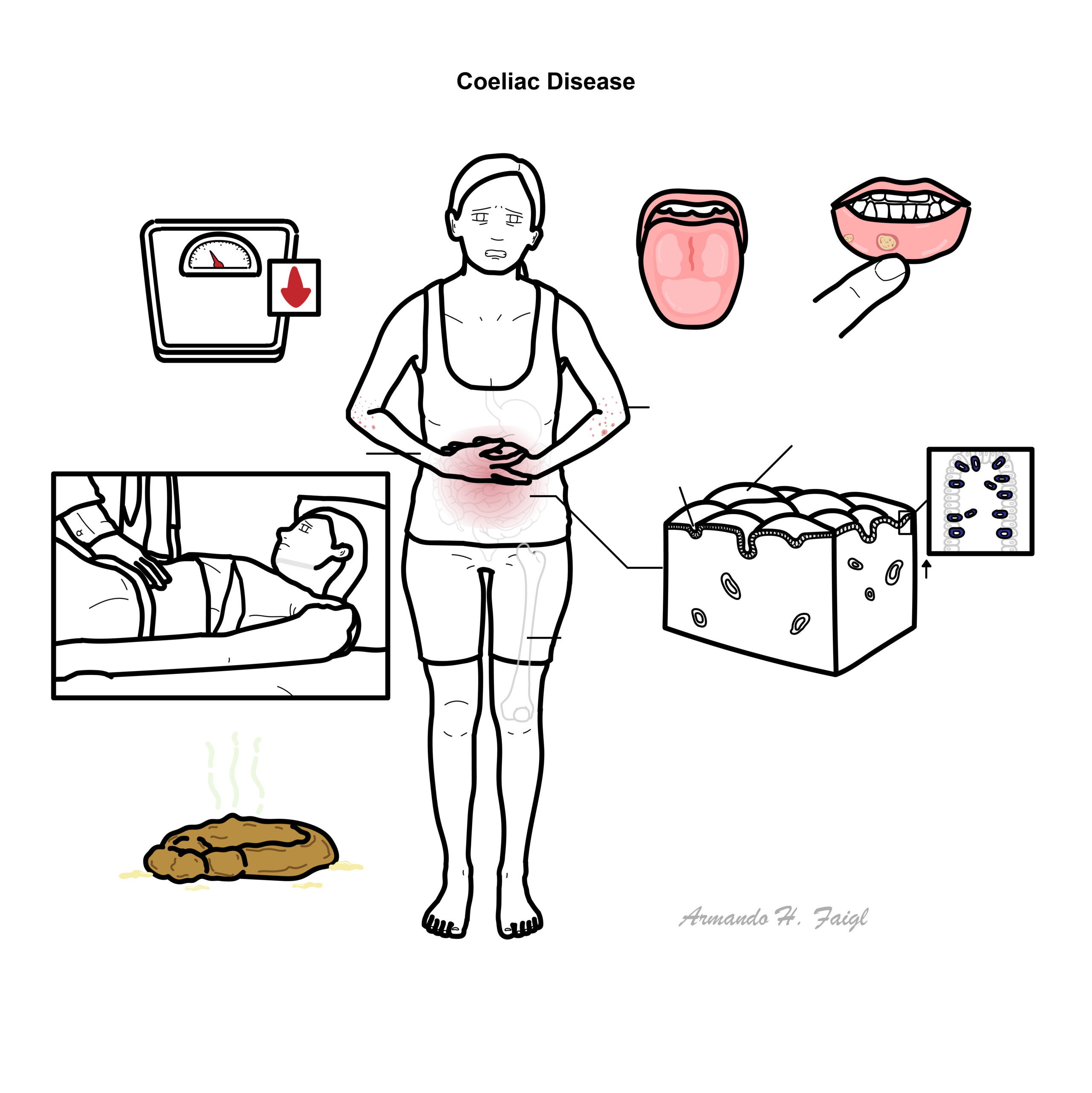
Clinical Manifestation
Clinical Presentation
- Asymptomatic (1/3)
- Stinking stools/steatorrhoea
- Diarrhoea
- Bloating
- Abdominal pain and discomfort
- Anemia
- Weight loss
- Failure to thrive (children)
Coeliac disease is associated with Type II diabetes (10%) and Genetic disorders such as Down’s Syndrome (12%).
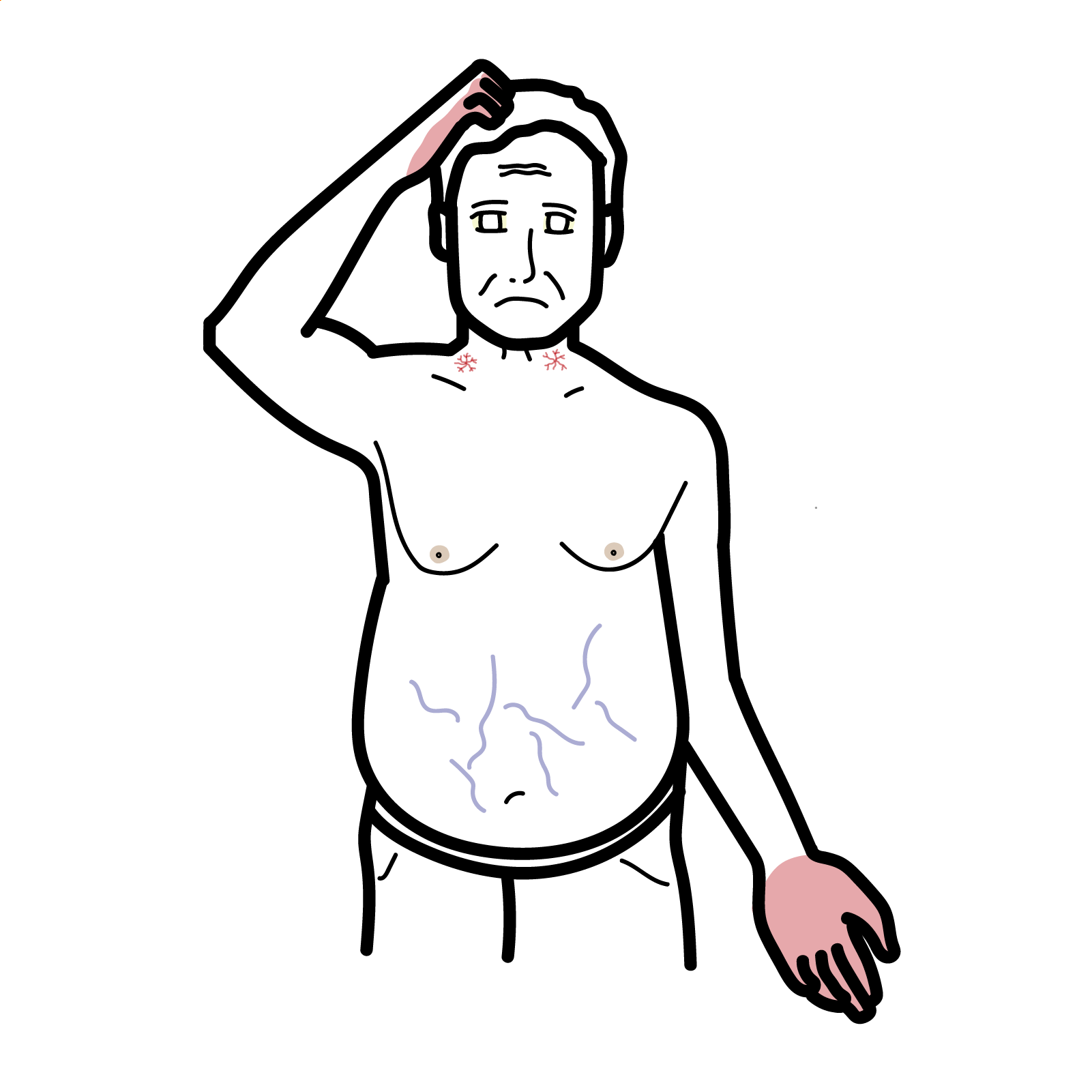
Clinical Examination – Usually normal, signs are seen in severe cases
- Anorexia
- Delayed puberty
- Atrophic glossitis
- Dermatitis herpitaformis
- Apthanous ulcers
- Osteopenia/osteoporosis
Suspect Coeliac Disease in all those with diarrhoea + weight loss or anaemia (esp. if iron or B12).
Differential Diagnosis
Childhood other food-sensitive enteropathies (milk sensitivity)
Adults
- Lymphoma
- Whipple’s disease
- Crohn’s Disease
- Giardiasis
- Irritable Bowel Syndrome
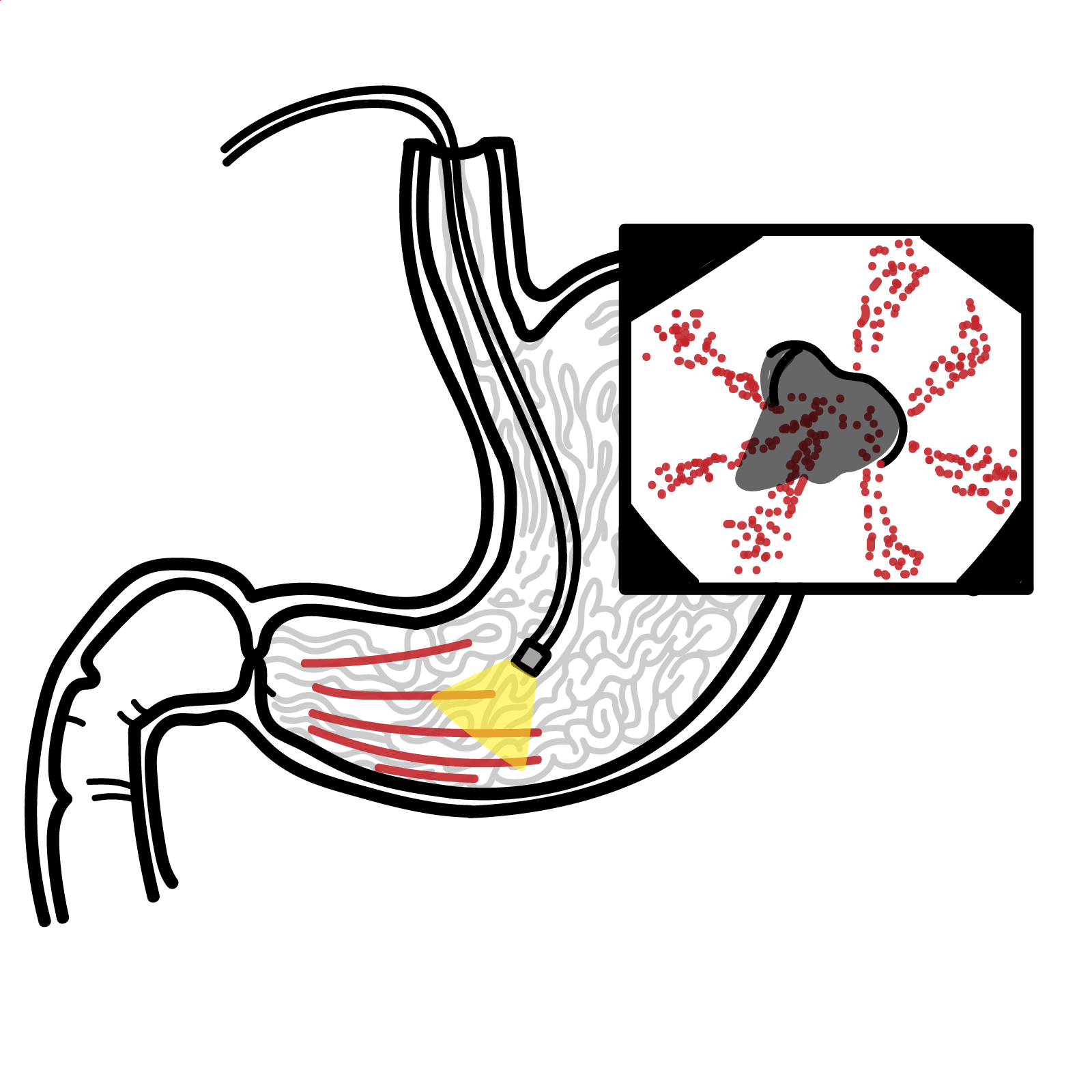
Investigations
- Serology
- Immunoglobin A-tissue transglutaminase (IgA-tTG)
- Endomysial antibody
- α-Gliadin antibody
- FBC – Low blood count
- Blood smear – Microcytic anemia due to folate deficiency
- Small bowel histology
- HLA testing (HLADQ2 & HLADQ8)
- Endoscopy
- Gluten Challenge – patients consume gluten diet and serological tests and small bowel histology is obtained 2-8 weeks after.
Exclude coeliac disease in all diagnosed with irritable bowel syndrome.
Diagnosis Small Bowel Histological changes including:
- Villous atrophy
- Hypertrophy of the intestinal crypts
- Increased numbers of lymphocytes in the epithelium and lamina propria
Treatment
General
- Gluten free diet
- Calcium supplement
- Vitamin Supplement
- Iron supplement
Coeliac crisis management – Medical Emergency
- Rehydration
- Electrolytes
- Corticosteroids
Complications and Prognosis
- Anaemia
- 2° lactose-intolerance
- GIT-cell lymphoma
- Malignancy (gastric, oesophageal, bladder, breast, brain)
- Myopathies
- Neuropathies
- Hyposplenism
- Osteoporosis
- Dermatitis herpetiformis
Dermatitis Herpetiformis: Very itchy/“burning” blisters on elbows, scalp, shoulders, ankles

- Gluten-free diet can have a normal life expectancy
- Adults with coeliac disease have an increased incidence of carcinoma in a number of sites. The risk reduces after gluten withdrawal. J
References
A Colour Handbook of Gastroenterology
Oxford Clinical Handbook of Clinical Medicine
Sleisenger and Fordtran’s Gastrointestinal and Liver Disease 10th Ed.






Members only discussions coming soon…