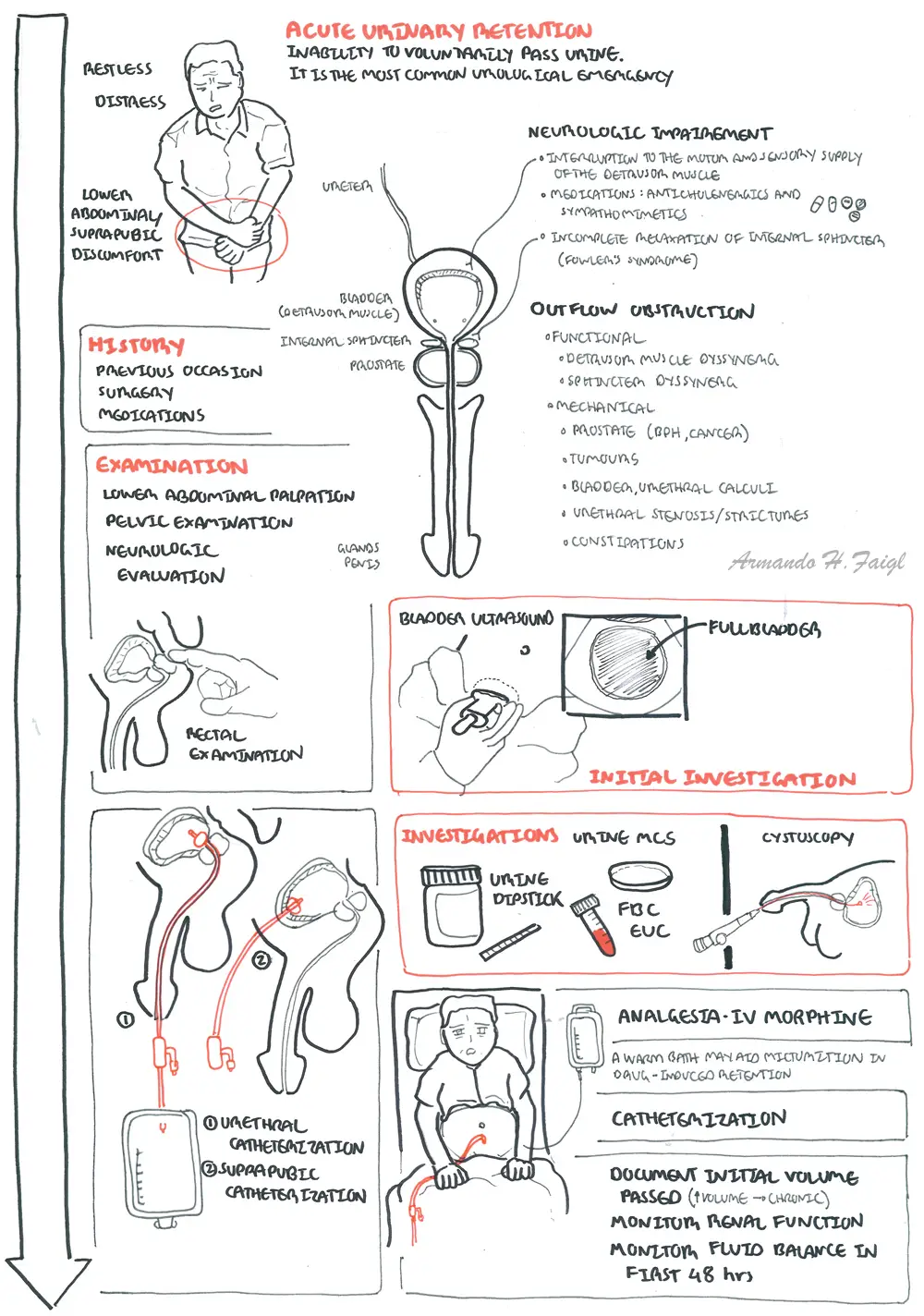
Acute Urinary Retention

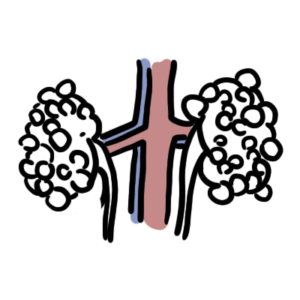
Acute urinary retention (AUR) is the inability to voluntarily pass urine. It is the most common urologic emergency. In men, AUR is most often secondary to benign prostatic hyperplasia. Acute urinary retention is rare in women.
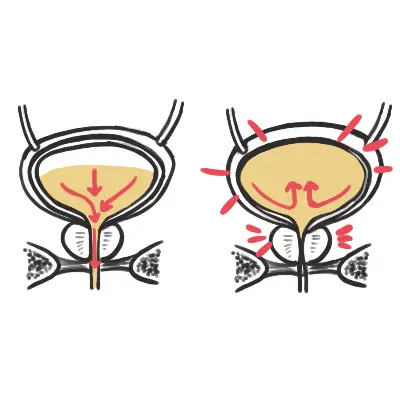
Pathogenesis
| CLASSIFICATION OF URINARY RETENTION | |
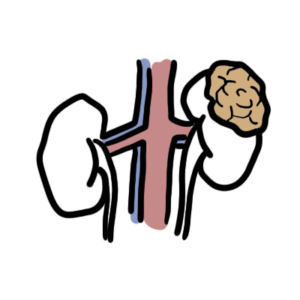
| Obstruction | Benign prostatic hyperplasia (BPH). Other causes of outflow obstruction in men include constipation, cancer (prostate or bladder), urethral stricture, urolithiasis, phimosis, or paraphimosis |
| Neurological Disease | Spinal cord injuries from trauma, infarct or demyelination, epidural abscess and epidural metastasis, Guillain-Barré syndrome, diabetic neuropathy, and stroke |
| Medications | Anticholinergic and sympathomimetic drugs |
| Infections | Infections may lead to AUR in the setting of inflammation that causes obstruction. For example, an acutely-inflamed prostate gland from acute prostatitis |
| Trauma | Trauma to the pelvis, urethra, or penis |
| COMMON CAUSES OF ACUTE URINARY RETENTION BASED ON GENDER | |||
| Condition | History | Examination | |
| MEN | Prostate Cancer | Weight loss, constitutional signs and symptoms | DRE: enlarged nodular (hard) prostate |
| Benign Prostatic Hyperplasia | Nocturia, frequency, polyuria, hestitency, double voiding | DRE: enlarged firm, non-tender, non-nodular prostate | |
| Acute Prosatitis | Dysuria, Fever | DRE: tender, boggy prostate | |
| Phimosis, Paraphimosis | Pain and swelling of foreskin or penis | Oedema of penis with nonretractable foreskin | |
| WOMEN | Vulvovaginititis | Vaginal Discharge, itch, dysuria | Vaginal discharge, inflamed genital area |
| Cystocele | Feeling of pelvic heaviness or fullness, noticeable bulge from the vagina. | Notable bulge on the anterior vaginal wall | |
| Pelvic mass (fibroids, gynaecological malignancy) | Feeling of pelvic heaviness or fullness, dysmenorrhea, menorrhagia | Palpable uterine mass | |
| BOTH GENDERs | Urinary Tract Infection | Dysuria, haematuria, groin/loin/back pain, genital rash | Supracpubic tenderness, urethral discharge, genital rash |
| Bladder Tumour | Painless haematuria with clots | – | |
| Neurogenic Bladder | Diagnosed neurological disease | Other generalised or focal neurologic deficits | |
| Rememeber Faecal impaction in the elderly may be a cause of urinary retention. |
| Rememeber Digital rectal examination is mandatory in the patient with new retention. |
Acute urinary retention should be managed by immediate and complete decompression of the bladder through catheterization.
| Remember Catheterization Contraindications: urethral disruption, posteoperative urological patients, known stricture. |
Complication of decompression
More Info on Haematuria










Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion