Chagas Disease


Authors
Megan Miner
Armando Faigl
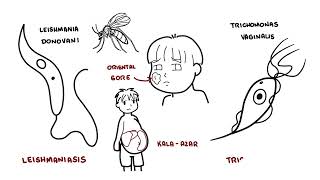
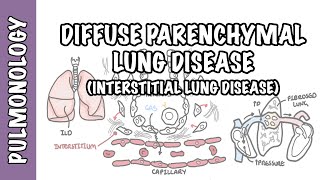
Chagas disease is caused by the parasitic protozoan Trypanosoma cruzi (T. cruzi) and is potentially life-threatening. These parasites often live within triatomine bugs. Following a bite to the skin, these bugs, also known as “kissing bugs”, deposit fecal matter near the site of the bite. Their bite, unfortunately, causes the person to scratch, thus allowing the fecal matter (and T. cruzi parasite) to enter systemic circulation, thus, causing the disease. There are two stages to Chagas disease, acute and chronic.
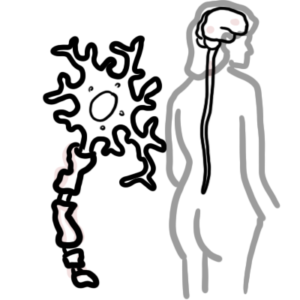
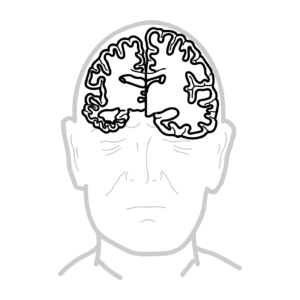
Triad for chronic Chagas disease: cardiomegaly, enteromegaly, and neurological symptoms.
Chagas Disease: Disease resulting from the T. cruzi parasite.
Trypanosoma cruzi: A parasitic protozoan that lives, typically, in the triatomine bug
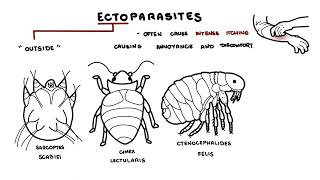
Triatomines: An insect that carries the T. cruzi parasite
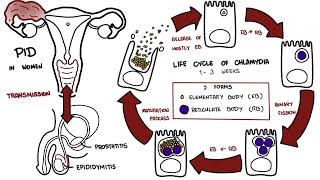
Life Cycle of Trypanosoma cruzi
Chagas disease and its associated symptoms are caused by the T. cruzi parasite and is transmitted to humans via triatomine bugs.
Other routes of transmission:
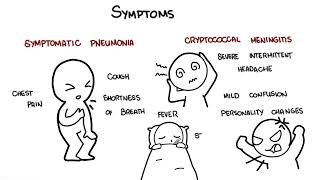
Acute Chagas’ disease is usually an illness of children. During the acute phase, many may display viral symptoms. An inflammatory lesion called a chagoma develops at the site of entry. Romana’s sign (painless periorbital oedema) may be seen if the site of entry is the conjunctiva.
Innate immunity increases cytokine and chemokine production in response to the parasitic infection. The adaptive immune system produces B cells, T cells, and antibodies. Gradually, parasite levels drop, and the patient enters an asymptomatic phase. The person now enters the intermediate phase. There is no sign of the parasite, except for IgG produced against T. cruzi.
Severe myocarditis with CCF may occur in the acute phase.
After the acute phase patients enter the asymptomatic phase. There is no sign of the parasite, except for IgG produced against T. cruzi. Years later chronic chagas disease can reemerge.
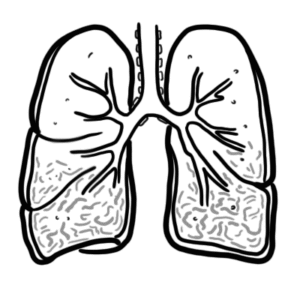
About 30% of people will develop the chronic phase of Chagas disease 15-30 years after being bitten. The main organs affected is the heart or the gastrointestinal tract.
Specifically in the heart, Chagas disease results in:
Chronic Chagas’ disease is diagnosed by detection of IgG antibodies to the parasite in the presence of clinical symptoms.
Patients with chronic Chagas disease (including those with cardiomyopathy) have a poor prognosis. However, many live with the disease unbeknownst to them. Likewise, early intervention with medication provides patients with an optimistic prognosis.
Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.












Discussion