Chronic Pancreatitis


Chronic pancreatitis is characterised by recurrent or persistent abdominal pain arising from the pancreas. The inflammatory process results in irreversible destruction and fibrosis of the pancreas. Often associated with exocrine or endocrine pancreatic insufficiency.
Acute Pancreatitis: An inflammatory process in which pancreatic enzymes are activated and cause autodigestion of the gland.
Chronic Pancreatitis: Irreversible damage causing fibrosis and scarring to the pancreas, resulting in exocrine and endocrine dysfunction
Pancreatic pseudocyst: Cystic space within the pancreas not lined by epithelial cells, often associated with chronic pancreatitis.
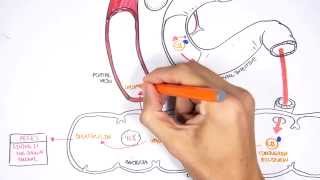
Pancreatic anatomy
Pancreas extends retroperitoneally across posterior abdominal wall. It means “All (pan) Flesh (Kreas)”. The pancreas consists of the following parts:
The head is encircled by duodenum and tail in contact with spleen. Pancreas has a poorly developed capsule & therefore adjacent structures (common bile duct, duodenum, splenic vein, transverse colon) are commonly involved in inflammatory process.
Blood Supply
Venous drainage
Nerve invervation
Embryology
Pancreatic physiology exocrine (98%) & endocrine (2%) functions
Exocrine: Pancreatic acinar cells produce digestive enzymes, which are stored in secretory granules. The Pancreatic exocrine secretion is regulated by cephalic, gastric & intestinal stimuli. Acinar cells secrete pancreatic juice made up the enzymes:
Exocrine section is stimulated by:
Endocrine: Islets of Langerhans – clusters of hormone-producing cells secreted directly into circulation. Endocrine cells of the pancreas:
| Cells of the Pancreas | Secretion | Function |
| Acinar cells secrete enzymes into the duodenum | Nucleases | Breaksdown nucleotides |
| Proteases | Digests Proteins | |
| Lipases | Digests lipids | |
| B-amylase | Digests carbohydrates | |
| Islets of Lagerhan secrete hormones into the bloodstream | Glucagon | Stimulates glucose release into the bloodstream from glucose stores |
| Insulin | Increases cell uptake and storage of glucose |
| Risk Factors |
| Alcohol |
| Smoking |
| Family history |
| Coeliac disease |
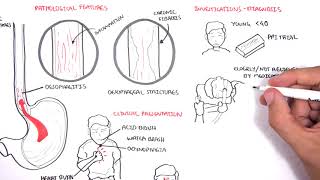
Pathological features
Clinical Presentation of chronic pancreatitis is similar to acute pancreatitis but less severe. This include epigastric pain that may radiate to the back, nausea and vomiting. Patients may present to ED and require opiates. Pain is worse with food and alcohol. Exocrine features of chronic pancreatitis include weight loss and malnutrition (due to malabsorption of macromolecules) and also steatorrhea (due to fat malabsorption).
Management involve prevention of cause/progressive damage by stoping alcohol and smoking. Encourage diet rich in antioxidant. Controlling symptoms and complication involve dietary modification (low fat), pancreatic enzyme supplements, analgesia (may require opiates), insulin (for diabetes if develops). Surgical management includes percutaneous or endoscopic drainage to drain excess fluid in the pancreas that is causing obstruction. Pancreaticduodenectomy is performed to remove possible causes and complications.
Resectional surgery is associated with increasing risk of exocrine and endocrine pancreatic failure and high risk of complications
Complications
UpToDate
Best Practice
Oxford Handbook of Clinical Medicine
Oxford Handbook of Clinical Surgery











Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion