

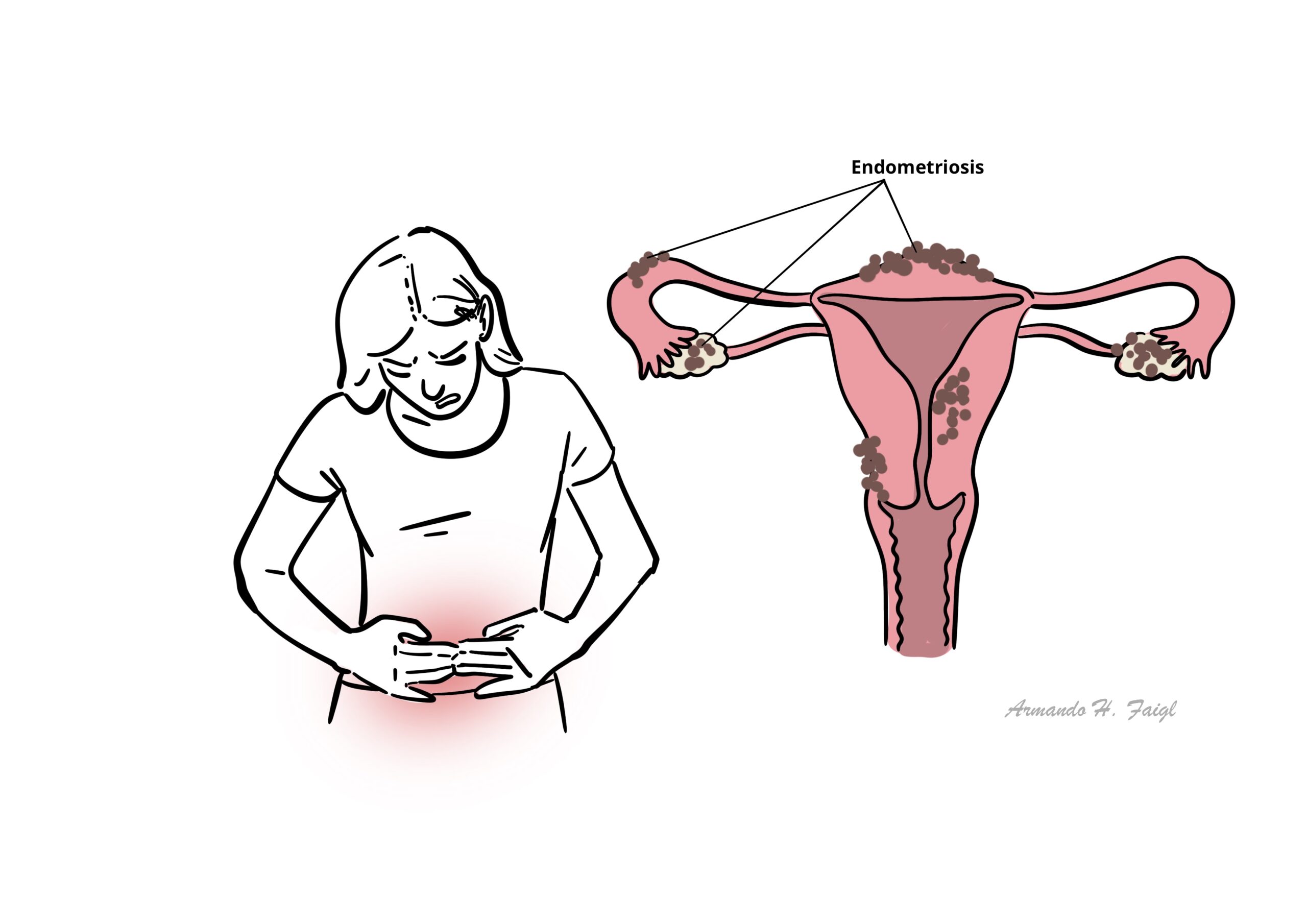
Endometriosis

A healthy 25-year-old woman presents with worsening dysmenorrhea, pain of recent onset in the left lower quadrant, and dyspareunia. She has regular menstrual cycles, and her last menstrual period was 3 weeks before presentation. She has been trying to fall pregnant over the past 10 months without success and she is becoming more concerned.
Overview
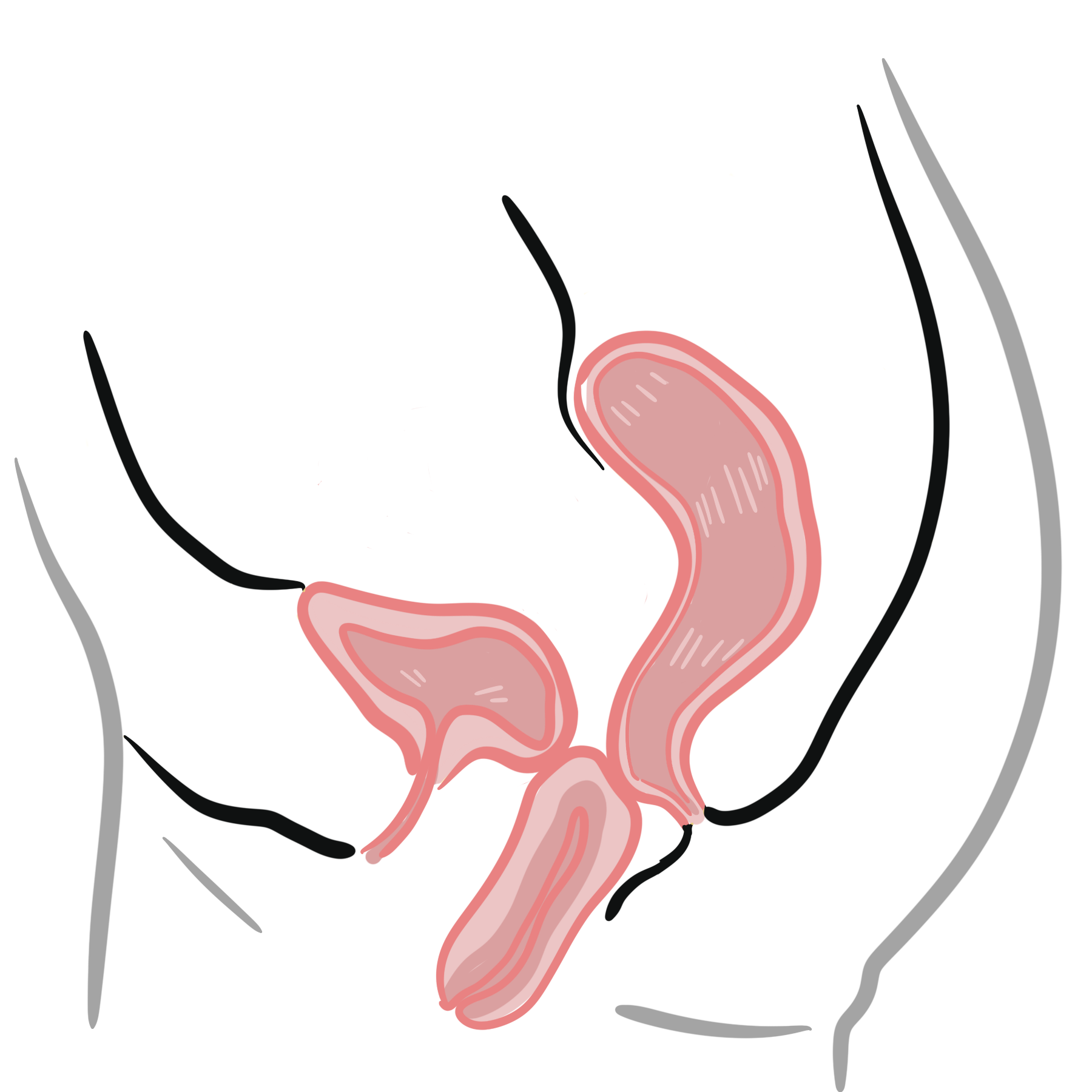
Endometriosis is defined as the presence of endometrial glands and stroma outside the endometrial cavity and uterine musculature. Like the endometrial tissue from which it is derived, endometrial implants and cysts respond to the hormonal fluctuation of the menstrual cycle. Endometriosis is a common condition associated with infertility and should be suspected in any infertile woman. Endometriosis affects 6-10% of women of reproductive age and is a major contributor to pelvic pain.
Definition
Endometriosis: The presence of endometrial glands and stroma outside the endometrial cavity and uterine musculature
Endometritis: Inflammation of the endometrium usually by an infection
Infertility: Inability to conceive after 1 year of unprotected intercourse.
Primary Infertility: A woman has never been able to get pregnant.
Secondary Infertility: A woman has been pregnant in the past, but has 1 year of inability to conceive.
Dysmenorrhoea: Painful menstruation
Dyspareunia: Difficult or painful sexual intercourse.
Risk Factors
- Mullerian anomiles
- Diethylstilbestrol exposure in utero
- Early Menarche
- Late menopause
- Obesity
- Short menstrual cycles
- Low birth weight
- Exposure to endocrine disrupting chemicals
- Genetics
- Red meat and trans fat
Protective factors include fruit, green vegetables, n-3 long chain fatty acids, prolonged lactation and multiple pregnancies.
Pathophysiology
Theories
- Retrograde menstruation
- Vascular and lymphatic dissemination of endometrial cells
- Coelomic metaplasia of multipotential cells in the peritoneal cavity
- Impaired Immunity
Clinical Manifestations
Clinical Presentation Women with extensive endometriosis may have minimal symptoms. Whereas, women with minimal endometriosis may have severe pain.
- Severe dysmenorrhea
- Chronic Pelvic pain
- Deep dyspareunia
- Ovulation pain
- Chronic fatigue
- Pain on defecation
- Infertility
Four Ds of endometriosis: dysmenorrhea, dyspareunia and dyschezia and dysuria.
Endometriosis should be considered a possible aetiology in patients who present with dysmenorrhea that does not respond to oral contraceptive or NSAIDs.
In approaching infertility, there are five basic factors to examine: (1) ovulatory, (2) uterine, (3) tubal, (4) male factor, and (5) peritoneal factor (endometriosis).
Clinical Examination
- Pelvic tenderness
- Fixed (immobile) retrograde uterus
- Tender/Thickened uterosacral ligaments which may be nodular
- Enlarged ovaries
Gyaenacological
- Adenomyosis
- Leiomyomata (Fibroids)
- Interstitial cystitis
- Pelvic Inflammatory Disease
- Ovarian cyst
- Uterine Myoma
Non-Gyaenacological
Investigations
- Transvaginal ultrasound (preferred)
- MRI
Diagnosis Laparoscopy is the “gold standard” in diagnosing endometriosis, and lesions may have a variety of appearances. The mean interval between the onset of pain and definitive surgical diagnosis is 10.4 years.
When surgical treatment is being considered, attempt laparoscopic excision or ablation at the time of diagnostic laparoscopy when possible.
| Indications for Laproscopy |
| NSAID – resistant lower abdominal pain/dysmenorrhoea |
| Pain resulting in days off work/school or hospitalization |
| Pain and infertility investigation |
Endometriosis is most commonly found on the ovaries and is typically bilateral.
Pathology
Gross and microscopic pathology Endometriosis lesions in the pelvis can be categorized into three types:
- Superficial peritoneal lesions – typically located on pelvic organ or pelvic peritoneum. Classical lesions are powder burn or gun shot lesions
- Ovarian lesions (endometrioma) – an ovarian cyst, or endometrioma, is formed when ectopic endometrial tissue within the ovary bleeds and results in a hematoma surrounded by duplicated ovarian parenchyma
- Deeply infiltrating endometriosis – a solid endometriosis mass situated more than 5 mm deep to the peritoneum
Treatment
General
- Simple analgesia:
- Paracetamol.
- NSAIDs for dysmenorrhoea and pelvic pain, if not contraindicated.
- Heat therapy, regular exercise and sleep optimisation.
- Pelvic-floor physiotherapy for pelvic-floor overactivity, dyspareunia or musculoskeletal pain.
- Psychological support and multidisciplinary pain management for chronic or centralised pain
Hormonal treatment – mimic pregnancy or menopause
- Combined oral contraceptives
- Progestagens
- Intrauterine Devices (Mirena)
- Gonadotropin-releasing hormone agonists
- Aromatase inhibitors
All drugs are equally effective in relieving pain and are associated with up to 50% recurrence after approximately 12-24 months after stopping.
Surgery
- Consider when:
- Symptoms remain severe despite adequate medical therapy
- Hormonal therapy is contraindicated or unacceptable
- Deep disease affects the bowel, bladder or ureter
- Fertility is affected in selected patients
- Usually performed laparoscopically:
- Excision or ablation of endometriotic lesions
Definitive surgery
- Hysterectomy ± removal of the ovaries may be considered for severe refractory symptoms when childbearing is complete
- All visible endometriosis should also be removed
- Hysterectomy is not guaranteed to cure pain, particularly when extrauterine disease or chronic pain sensitisation remains
In the five years after surgery or medical treatment, 20-50% of women will experience recurrence of symptoms.
Complications & Prognosis
- Chronic pelvic pain and severe dysmenorrhoea
- Deep dyspareunia
- Chronic fatigue and sleep disturbance
- Infertility or subfertility
- Pelvic adhesions and distortion of pelvic anatomy
- Ovarian endometriomas and reduced ovarian reserve
- Bowel, bladder or ureteric involvement:
- Bowel stenosis or obstruction.
- Ureteric obstruction and hydronephrosis.
- Haematuria or rectal bleeding.
- Rare extrapelvic disease, including diaphragmatic or thoracic endometriosis
- Reduced quality of life, sexual dysfunction, work or study impairment, anxiety and depression
- Pregnancy is possible, but endometriosis is associated with increased risks of ectopic pregnancy and first-trimester miscarriage; serious pregnancy complications remain uncommon
- Overall cancer risk is not substantially increased. There is a small absolute increase in certain ovarian cancers, particularly clear-cell and endometrioid ovarian carcinoma
- Endometriosis is a chronic, relapsing condition with no guaranteed permanent cure.
- Disease severity seen during surgery does not always correlate with pain severity.
- Many patients achieve good symptom control with hormonal treatment, surgery or combined multidisciplinary management.
- Symptoms often recur after hormonal therapy is stopped and may recur after surgery.
- Long-term postoperative hormonal suppression reduces recurrence when pregnancy is not immediately desired.
- Fertility prognosis depends on age, ovarian reserve, tubal function, disease extent, previous ovarian surgery and other infertility factors.
- Many patients conceive naturally or with fertility treatment.
- Symptoms frequently improve after menopause but may persist, particularly with residual disease or hormone therapy.
- Long-term prognosis is generally good regarding life expectancy; the main burden is recurrent pain, infertility and impaired quality of life.
References
- Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Australian Living Evidence Guideline: Endometriosis. Melbourne: RANZCOG; 2025.
- Becker CM, Bokor A, Heikinheimo O, Horne A, Jansen F, Kiesel L, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009.
- National Institute for Health and Care Excellence. Endometriosis: diagnosis and management. NICE guideline NG73. London: NICE; 2017. Updated 2024.
- Zondervan KT, Becker CM, Koga K, Missmer SA, Taylor RN, Viganò P. Endometriosis. Nat Rev Dis Primers. 2018;4(1):9. doi:10.1038/s41572-018-0008-5.
- Kvaskoff M, Mahamat-Saleh Y, Farland LV, Shigesi N, Terry KL, Harris HR, et al. Endometriosis and cancer: a systematic review and meta-analysis. Hum Reprod Update. 2021;27(2):393–420. doi:10.1093/humupd/dmaa045.








Members only discussions coming soon…