

Polyendocrine Metabolic Ovarian Syndrome
Overview
PMOS; formerly polycystic ovary syndrome—PCOS
In May 2026, PCOS was renamed polyendocrine metabolic ovarian syndrome (PMOS) to reflect its endocrine, metabolic, reproductive, dermatological and psychological effects. The terminology will transition gradually through to the 2028 international guideline update. It is not caused by multiple pathological ovarian cysts. Common chronic endocrine condition affecting approximately 10–13% of reproductive-aged women. Characterised by varying combinations of:
- Hyperandrogenism
- Ovulatory dysfunction
- Polycystic ovarian morphology
- Insulin resistance and metabolic dysfunction
Definition
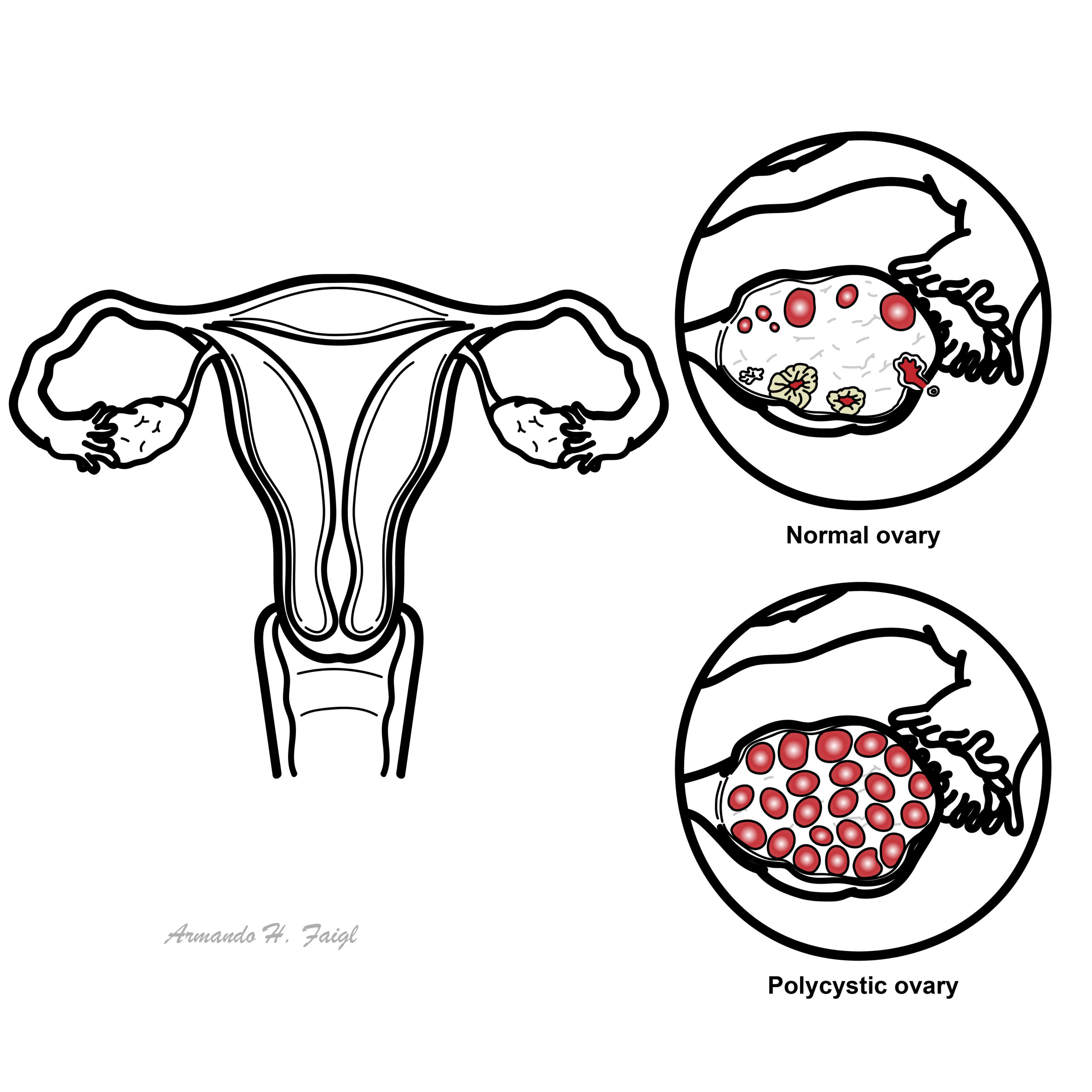
Cyst: A cyst is a sac or pocket in your body filled with fluid, semi-solid material or air
Ovarian cyst: Sac filled with liquid or semi-liquid material arising in an ovary. There are many differential diagnosis of ovarian cysts and majority are benign.
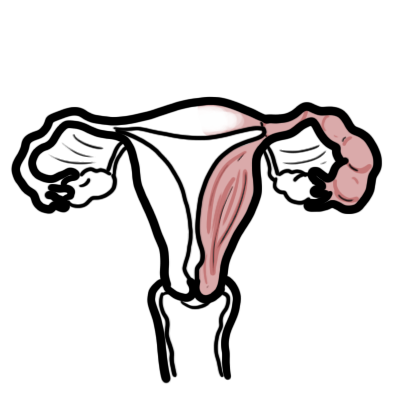
Anatomy & Physiology of Ovary
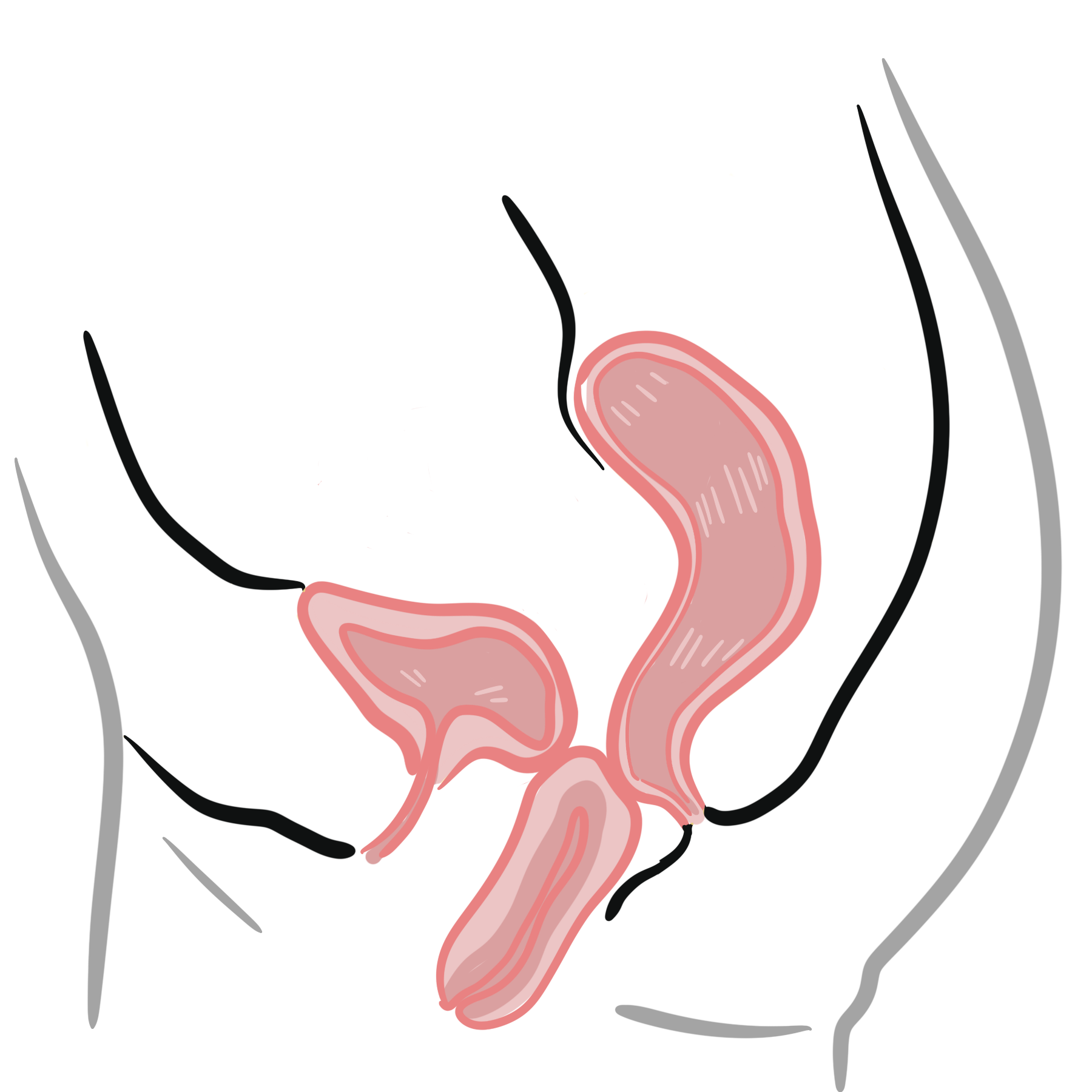
The Ovary
- Paired, situated on either side of the uterus
- Situated close to lateral pelvic wall
- Located in the ovarian fossa of Waldeyer
- The only intra-abdominal structure not covered by peritoneum
- Consists of the cortex and medulla
Ligaments associated with the Ovary
- Ovarian ligament – attaches to the ovary inferiorly and connects it to the uterus
- Suspensory Ligament of the Ovary – connect ovary to the lateral abdominal wall.
Blood supply
- Ovarian artery
- Right Ovarian vein: through pamipiniform plexus → Ovarian Vein → Inferior Vena Cava
- Left Ovarian Vein: through pamipiniform plexus → Ovarian Vein → Left Renal Vein → Inferior Vena Cava
Lymphatics
- Para aortic lymph nodes
Innervation
- Sympathetic supply from T10 along ovarian artery
Risk Factors
Family history of PCOS
- 50% of first-degree relatives
Premature adrenarche – development of PCOS in 50% of cases
- Early adrenarche – ‘awakening’ of adrenal gland, sex hormones causing changes such as development of pubic hair, oily skin, oily hair, body odour (development of apocrine sweat glands).
Early adrenarche differs to puberty. Puberty is when body becomes capable of sexual reproduction, development of testes and ovaries → secondary sex characteristics.
Clinical Manifestations
Clinical Presentation is often of a young women who experiences irregular periods +/- weight gain/hirsutism.
Hyperandrogenism
- Acne
- Hirsutism – hair
Menstrual disturbance
- Oligomenorrhoea
- Secondary amenorrhoea
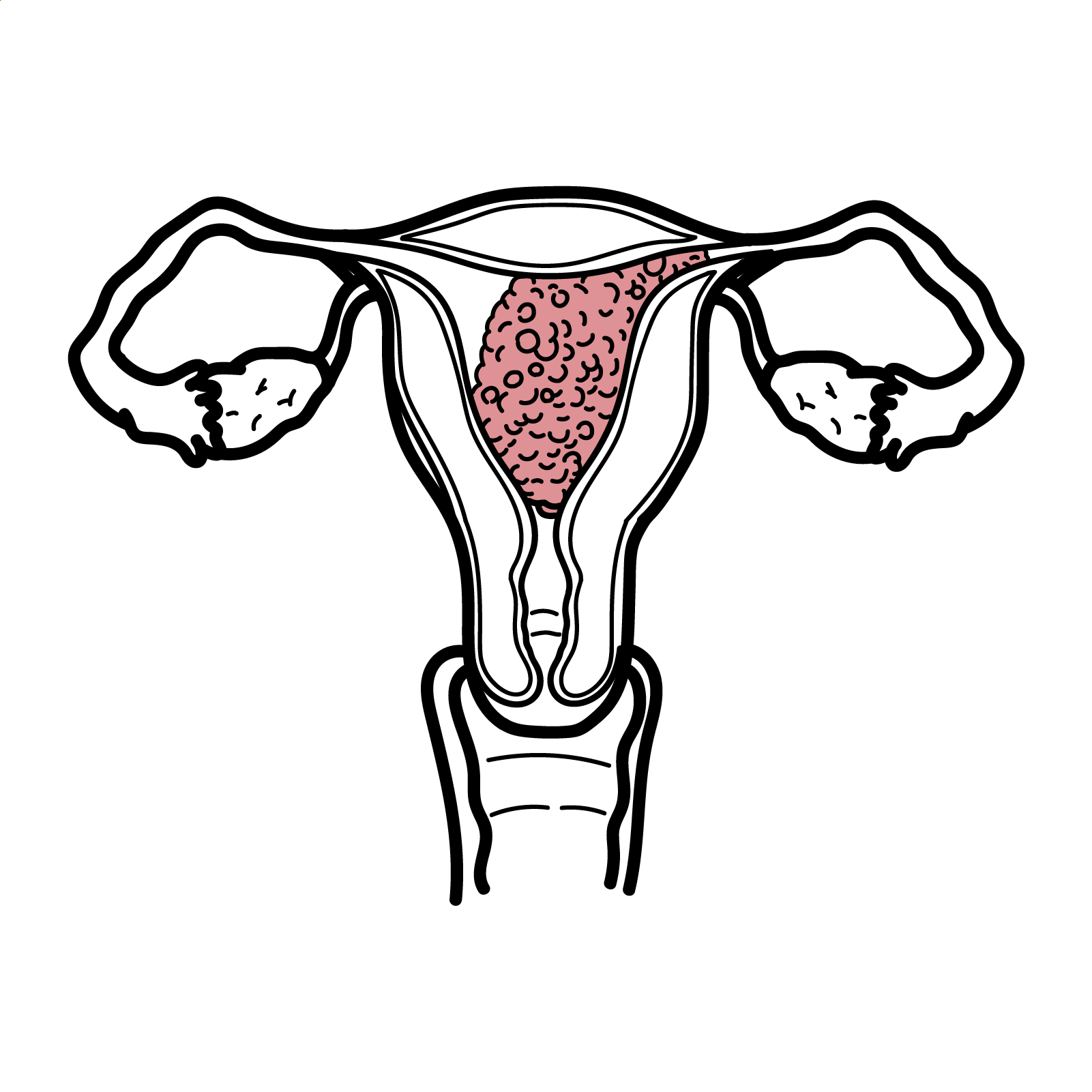
- Cystic ovaries
- Infertility
- Hyperglycaemia
- Elevated oestrogens
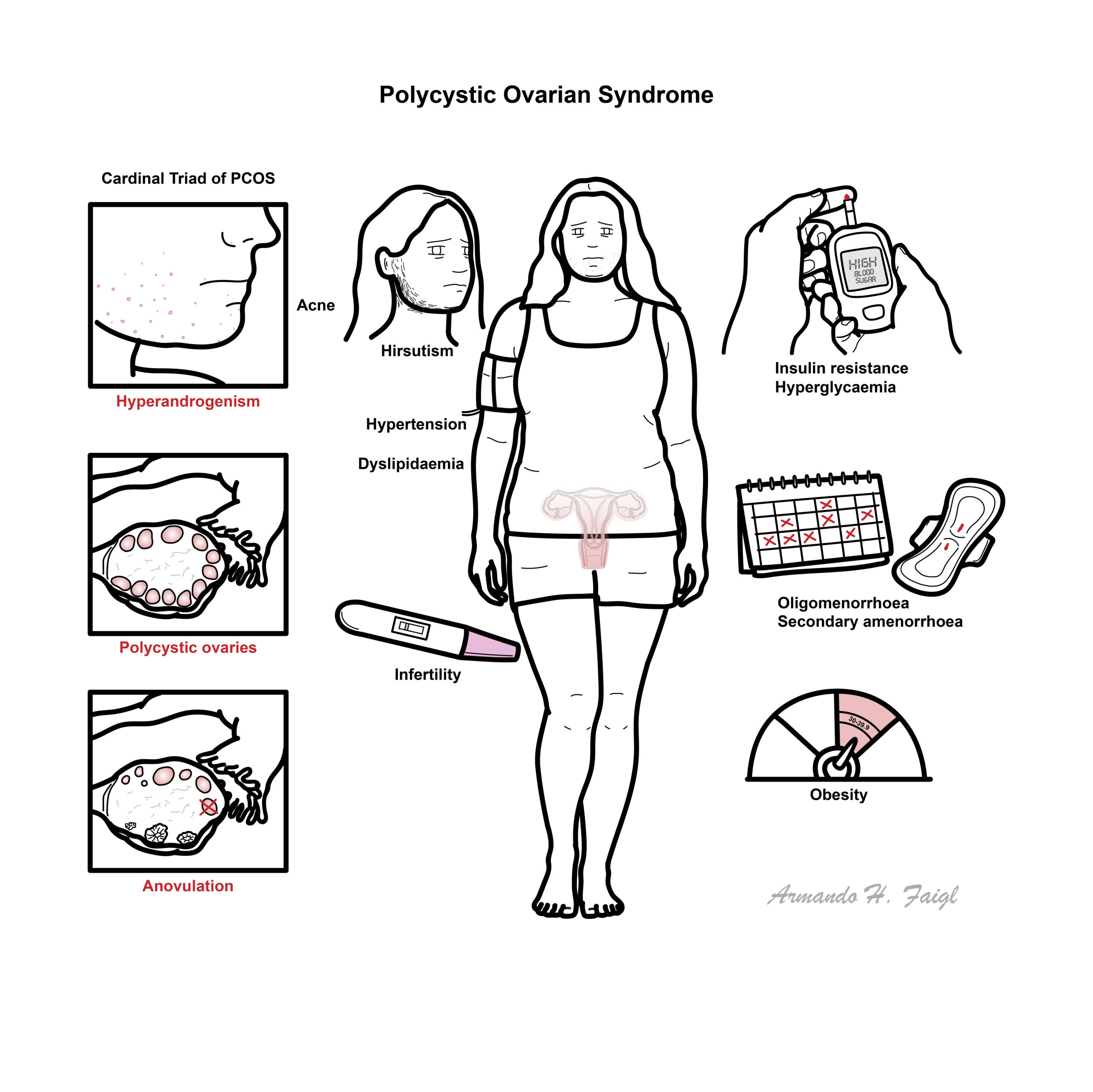
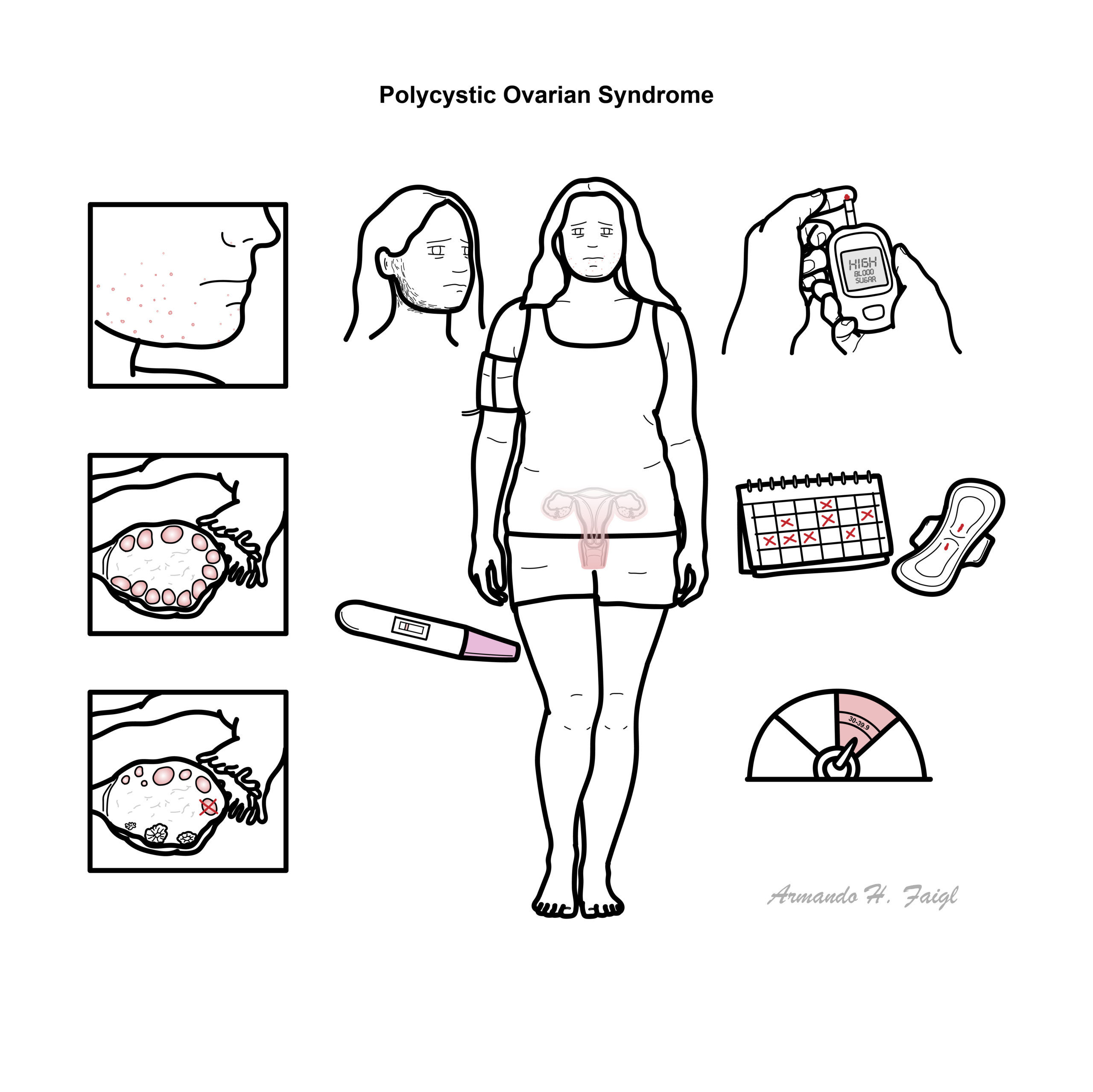
Cardinal Triad of PCOS: hyperandrogenism, presence of cysts in ovaries (>12) and anovulation.
Diagnosis
Diagnostic criteria in adults
Diagnosis generally requires two of the following three, after excluding alternative causes:
- Ovulatory dysfunction
- Irregular menstrual cycles
- Oligomenorrhoea or amenorrhoea
- Clinical or biochemical hyperandrogenism
- Hirsutism, acne or androgenic alopecia
- Elevated total or free testosterone
- Polycystic ovarian morphology
- Pelvic ultrasound, or
- Elevated AMH as an alternative to ultrasound in adults
If both irregular cycles and hyperandrogenism are present, ultrasound or AMH is usually unnecessary. AMH should not be used as a stand-alone diagnostic test
- Pregnancy test where appropriate
- Total and free testosterone or calculated free androgen index
- Androstenedione and DHEAS if testosterone is normal but suspicion remains
- TSH
- Prolactin
- 17-hydroxyprogesterone to exclude non-classic congenital adrenal hyperplasia
- Consider cortisol testing for suspected Cushing syndrome
- FSH ± oestradiol if premature ovarian insufficiency or hypothalamic amenorrhoea is suspected.
- 75-g oral glucose tolerance test: most accurate assessment of glycaemic status
- Lipid profile
Differential Diagnosis
- Congenital adrenal hyperplasia
- Hypothyroidism
- Hyperprolactinaemia
- Cushing’s syndrome
Congenital adrenal hyperplasia refers to enlarged adrenal glands. It is due to inherited enzyme deficiency. Congenital adrenal hyperplasia is the most common adrenal disorder of infancy and childhood.Congenital adrenal hyperplasia results excessive androgens (male hormones). There is also a severe salt-losing form of the condition.
Differential Diagnosis for Ovarian Cysts
- Polycystic Ovarian Syndrome
- Endometriomatous Cysts
- Function cysts – most common
- Follicular cysts
- Theca luthein cysts
- Corpus luteum cysts
Endometriomatous cysts of the ovary are cysts filled with blood arising from the ectopic endometrium. They usually enlarge pre and during menses and slightly shrink thereafter. The ovary is the commonest site of pelvic endometriosis.
Treatment
Lifestyle management
- Healthy eating, physical activity and behavioural support.
- Weight loss if overweight
- No single diet or exercise program has been proven superior.
Irregular periods and endometrial protection
- Combined oral contraceptive pill: first-line for irregular cycles and hyperandrogenism when pregnancy is not desired.
- Cyclic oral progestogen if amenorrhoeic and oestrogen-containing contraception is unsuitable.
- Progestogen-only contraception or levonorgestrel intrauterine device may provide endometrial protection.
Hirsutism and acne
- Combined oral contraceptive pill.
- Cosmetic therapies:
- Laser or light therapy
- Electrolysis
- Mechanical hair removal
- Consider an anti-androgen after at least six months of inadequate response:
- Spironolactone is commonly used.
Metabolic features
- Metformin: primarily for insulin resistance, impaired glucose tolerance and other metabolic features, particularly with BMI ≥25 kg/m² or increased diabetes risk.
- Start at a low dose and gradually titrate to reduce gastrointestinal adverse effects.
- Treat diabetes, hypertension and dyslipidaemia according to standard guidelines.
- Anti-obesity medication, including GLP-1 receptor agonists
- Bariatric/metabolic surgery may be considered in appropriately selected patients.
Infertility
- Optimise weight, blood pressure, diabetes risk, smoking, alcohol and folate before conception.
- Letrozole: first-line pharmacological ovulation induction for anovulatory infertility without other infertility factors.
- Alternatives:
- Clomiphene citrate
- Clomiphene plus metformin
- Metformin alone, although less effective than other ovulation-induction agents
- Second-line:
- Gonadotrophins
- Laparoscopic ovarian surgery in selected patients
- IVF if oral and second-line ovulation-induction treatments fail or another infertility factor is present.
- Patients undergoing IVF have an increased risk of ovarian hyperstimulation syndrome.
Psychological and associated conditions
- Treat depression, anxiety and eating disorders according to usual guidelines.
- Consider psychological therapy, including cognitive behavioural therapy.
- Treat obstructive sleep apnoea when identified.
Complications & Prognosis
- Infertility
- Pregnancy complication (ie. spontaneous pregnancy loss)
- Type 2 Diabetes
- Non-alcoholic fatty liver disease
- Cardiovascular disease
- Obstructive sleep apnoea
- Psychological issues
- Metabolic syndrome
- Dyslipidemia
- PMOS is a chronic but manageable condition with symptoms that vary between individuals and across life stages.
- Many patients achieve good menstrual, metabolic and dermatological control with appropriate long-term management.
- Pregnancy can often be achieved naturally or with ovulation induction or assisted reproduction.
- Reproductive symptoms may become less prominent with age, but diabetes and cardiovascular risk factors may persist.
- Long-term follow-up should include periodic assessment of glycaemia, blood pressure, lipids, menstrual regularity and psychological wellbeing.
- Regular cycle regulation or progestogen exposure substantially reduces the risk associated with prolonged unopposed oestrogen and amenorrhoea.
References
UptoDate
Best Practice








Members only discussions coming soon…