

Menopause

Overview
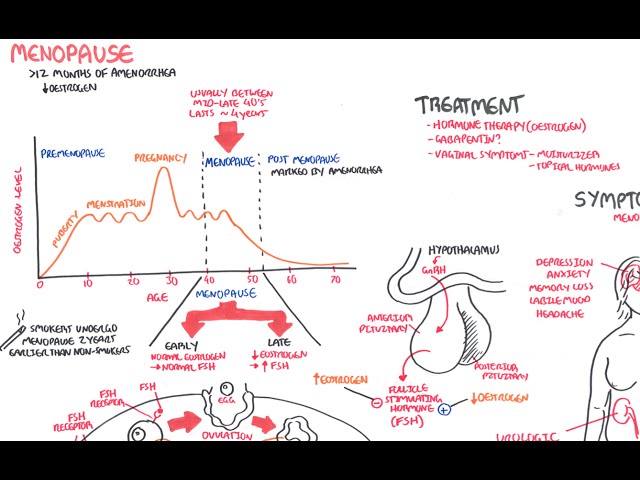
The menopause means the final menstrual period – diagnosed retrospectively after one year of amenorrhoea. Cessation occurs due to loss of ovarian function. The “declining oocyte pool” theory states that a newborn girl is born with millions of eggs, most of which die by atresia. The average age of menopause is 50, however this can vary widely between different cultures.
Definition
Menopause: is the last period, but the term is often used to cover the physiological cahages that occur around this time
Perimenopause: Period beginning with the first clinical biological, and endocrinological features of the approaching menopause
Premenipause: or menopause transition, begins several years before menopause.
Postmenopause: The last menstrual period
Premature ovarian failure: Cessation of menses for more than 1 year before 40 years of age, secondary to loss of ovarian function
Climactric: Phase encompassing the transition from the reproductive state to the non-reproductive state.
The term peri-menopause is synonymous with the climacteric. This is a phase of menstrual cycle irregularity, fluctuating hormone levels and symptoms associated with ovarian senescence. Lasts an average of 4 – 6 years before the final menstrual period to 1 year after the menopause.
Pathophysiology
Risk Factors
Menopause is a normal physiological process!
Clinical Manifestation
The most important clinical presentation is irregular periods or oligomenorrhoea.
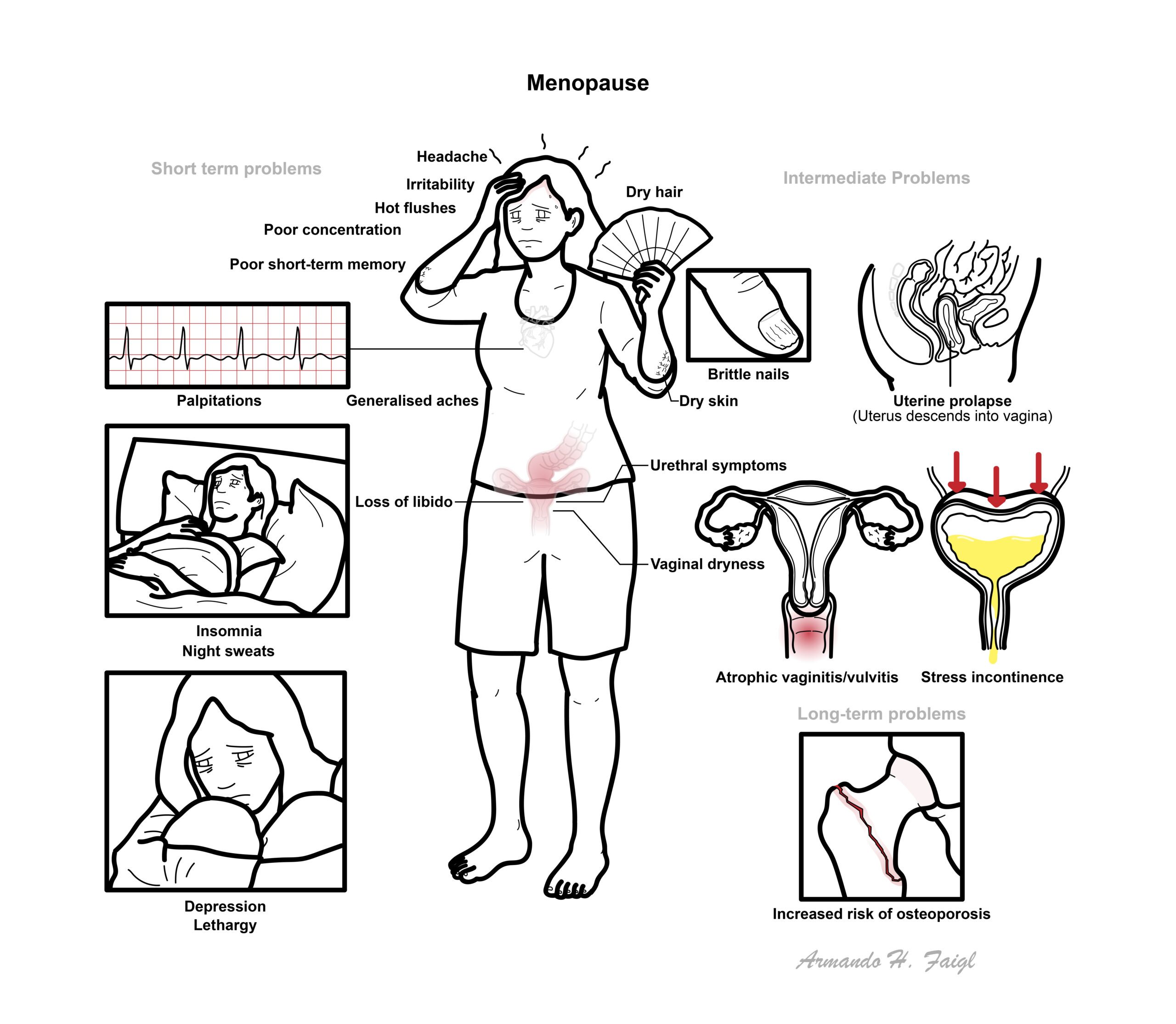
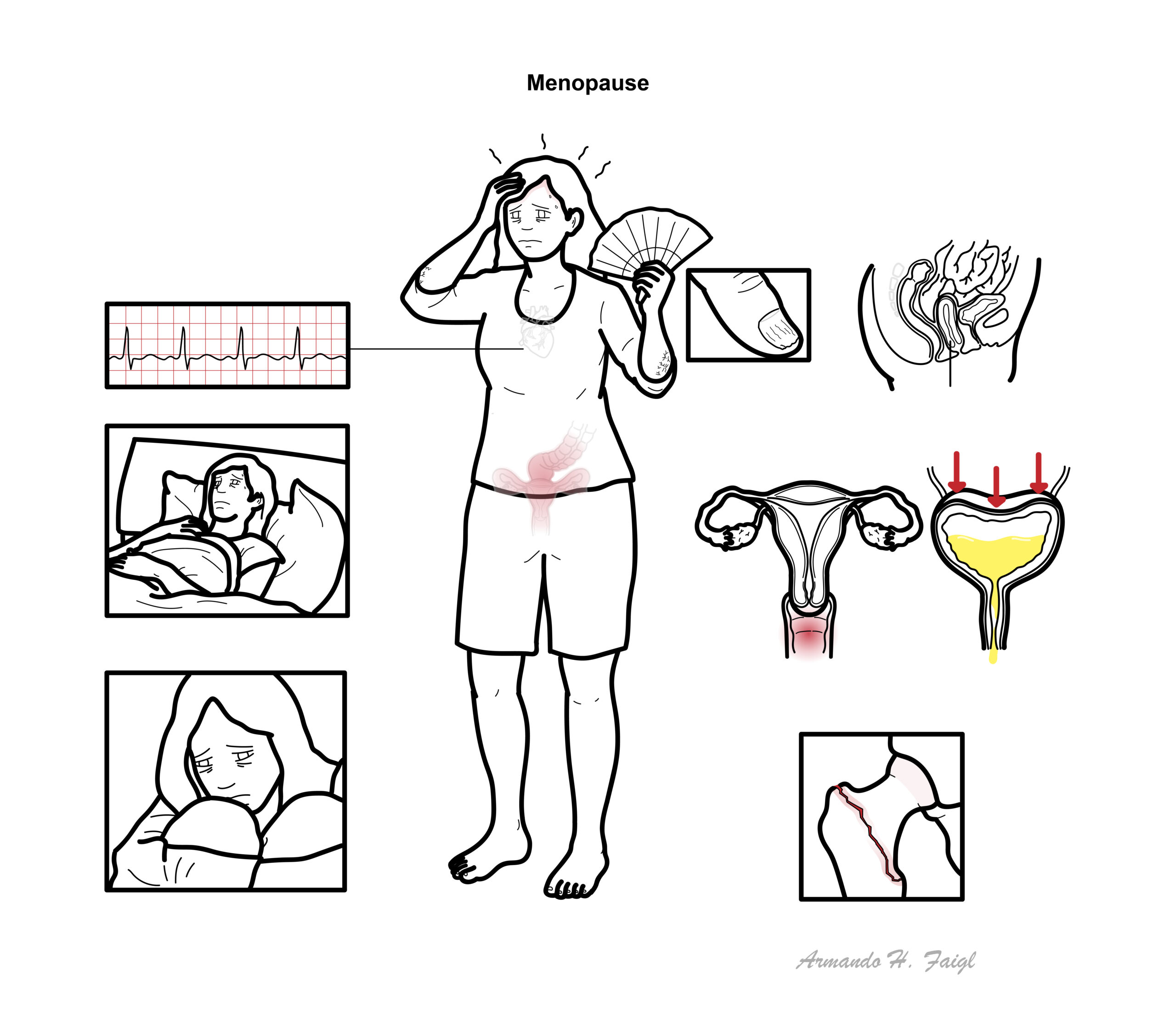
Short term problems
- headahce
- Hot flushes
- Night sweats
- Palpitations
- Insomnia
- Irritability
- Poor concentration
- Poor short-term memory
- Depression
- Lethargy
- Loss of libido
- Generalised aches
Intermediate Problems
- Urethral symptoms
- Uretine propase
- Stress incontinence
- Dyspareunia
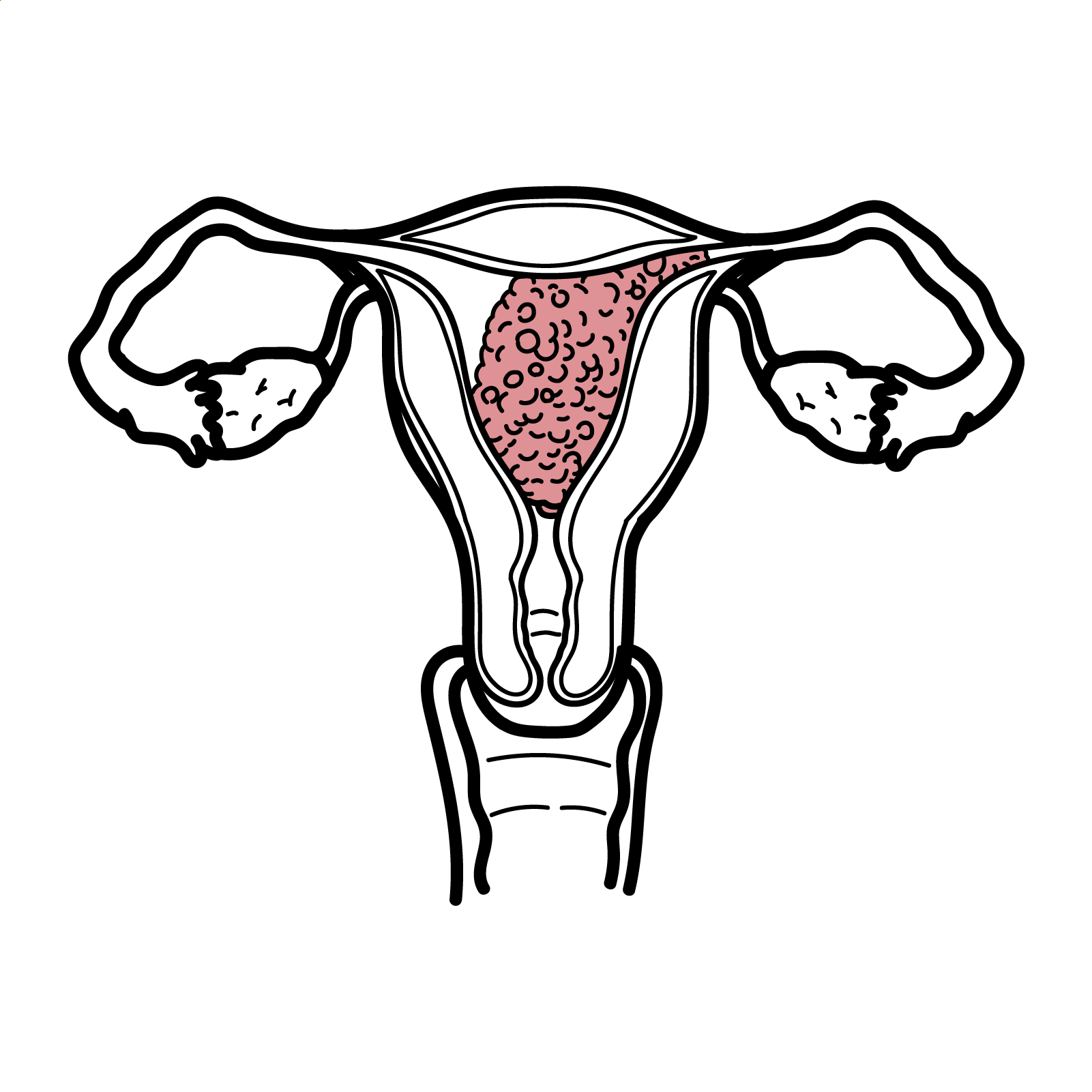
- Atrophic vaginitis/vulvitis
- Vaginal dryness
- Dry skin
- Dry hair
- Brittle nails
Long-term problems
- Cardiovascular disease
- Cerebrovascular disease
- Osteoporosis
Investigations
Investigation are usually unnecessary if women is of menopausal age. Investigations that could be considered:
- Thyroid function test
- Testosterone
- Bone mineral density
- Follicle stimulating hormone – if patient young age to rule out other causes of amenorrhoea
Treatment
Non-pharmacological
- Education
- Psychological support
Pharmacological treatment Oestrogen supplementation is the bases of replacement therapy. However, because of the long-term side effects of unopposed oestrogen often progesterone is also given. Oestrogen therapy (hormone replacement therapy) include:
- Oral preparations
- Transcutaneous administration
- Subcutaneous implants
- Vaginal preparations
Pharmacology
Hormone replacement therapy is ofference to treat menopausal symptoms and to reduce long-term hypo-oestrogen side effects. Adverse effects: Nausea/vomiting, Endometrial cancer, Breast cancer, Venous thrombolic disease, Stroke. Contraindication Venous thromboembolic disease, Pregnancy, liver disease.
Menopause & Alternative Medicine
Due to the risks involved with HRT, many women may prefer the perceived safety of complementary and alternative medicines in the management of menopausal symptoms.
Commonly used alternative medicines
- Pytooestrogens, present in many foods e.g. soy, legumes, other vegetables
- Black cohosh
- Red clover isoflavones
- Plant extracts e.g. Valeriana officinalis, Melissae officinalis and Humulus lupulus
The evidence
- Phytooestrogens (plant-derived substances that induce oestrogen-like effects)
- Isoflavones (most common; found in soy-beans); lignans; coumestans
- Some studies demonstrate a moderate effect, others don’t
- Evidence has been criticised for not being clinically significant
- Side effect profile and long-term safety uncertain
- Black cohosh (herb)
- No evidence suggesting clinical significance
- Other plant extracts
- Insufficient data
Effect on placebo on hot flushes over several months is usually around 50%.
Complications
Complications of low oestrogen (post menopause)
- Cardiovascular Disease
- Cerebrovascular Disease
- Osteoporosis
- Dementia
Complications of Prolonged HRT
- Stroke
- Thromboembolic disease
- Endometrial cancer
- Ovarian Cancer
- Colorectal Cancer
- Breast Cancer
Premature Ovarian Failure
Overview
Premature ovarian failure is the cessation of menses for more than 1 year before 40 years of age, secondary to loss of ovarian function. Affects approximately 1% of women. Patients with premature ovarian failure present similarly to women of normal menopausal age, with symptoms of: hot flushes, sleep disturbance, irritability, infertility and vaginal atrophy.
- Family history
- Exposure to chemotherapy or radiation
- Autoimmune disease
- Galactomsaemia
- Weak risk factors: hysterectomy, uterine artery embolisation, smoking (doubles the risk of POF), ovarian surgery
- Pregnancy
- PCOS
- Anorexia nervosa
- Strenuous exercise/emotional or physical stress
- Sheehan’s syndrome
- Turner’s syndrome
- Asherman’s syndrome
- Medication-induced amenorrhagia
- Hypothyroidism
Unlike those who present at normal menopausal age, women suspected of having POF should always have their hormone levels investigated.
Investigations
- Serum β-hcg: must always rule out pregnancy
- Serum FSH – elevated
- Serum LH – elevated
- Oestrodiol – low respectively
- Anti-Mullerian hormone (AMH): low in POF
- TFTs, including thyroid peroxidase antibodies, to check for autoimmune hypothyroidism (may be the cause)
- Serum prolactinaemia: hyperprolactinaemia is a common cause of secondary amenorrhoea – want to rule this out (should be normal in POF)
- Transvaginal ultrasound: will show small ovaries with minimal follicular activity in POF. Can help distinguish between other causes (e.g. PCOS, Asherman’s syndrome).
- Consider screening for diabetes (BSL), a karyotype study, and investigating for the FMR-1 gene mutation (Fragile X syndrome)
References
Macgowan, BA., Owen, P., & Thomson, A. (2014). Clinical Obstetrics & Gyaenacology. 3rd ed. Saunders Elsevier. London.
Oxford Handbook of Obstetrics and Gynaecology 3rd edition







Members only discussions coming soon…