

Endometrial Cancer

Overview
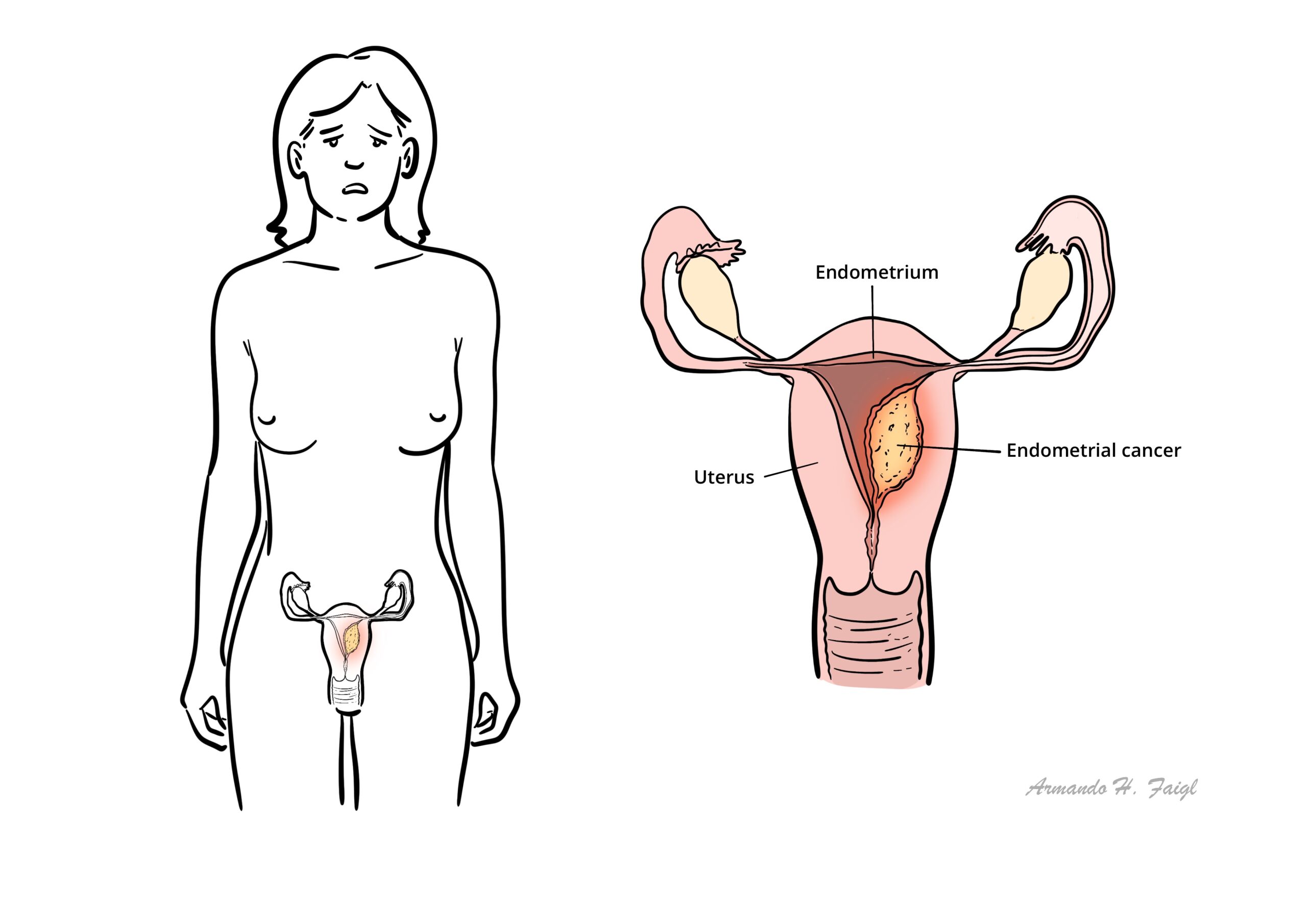
Endometrial carcinoma is an epithelial malignancy of the uterine corpus mucosa, usually an adenocarcinoma. Endometrial carcinoma is the most common female genital tract malignancy. Postmenopausal bleeding always needs to be investigated because it can indicate malignant disorders and premalignant conditions, such as endometrial hyperplasia. The most common etiology of postmenopausal bleeding is atrophic endometritis or vaginitis.
Definition
Menopause: Permanent cessation of menstrual periods, determined retrospectively after a woman has experienced 12 months of amenorrhoea without any other obvious pathological cause. The average age is 52, with a range between 45-55 years
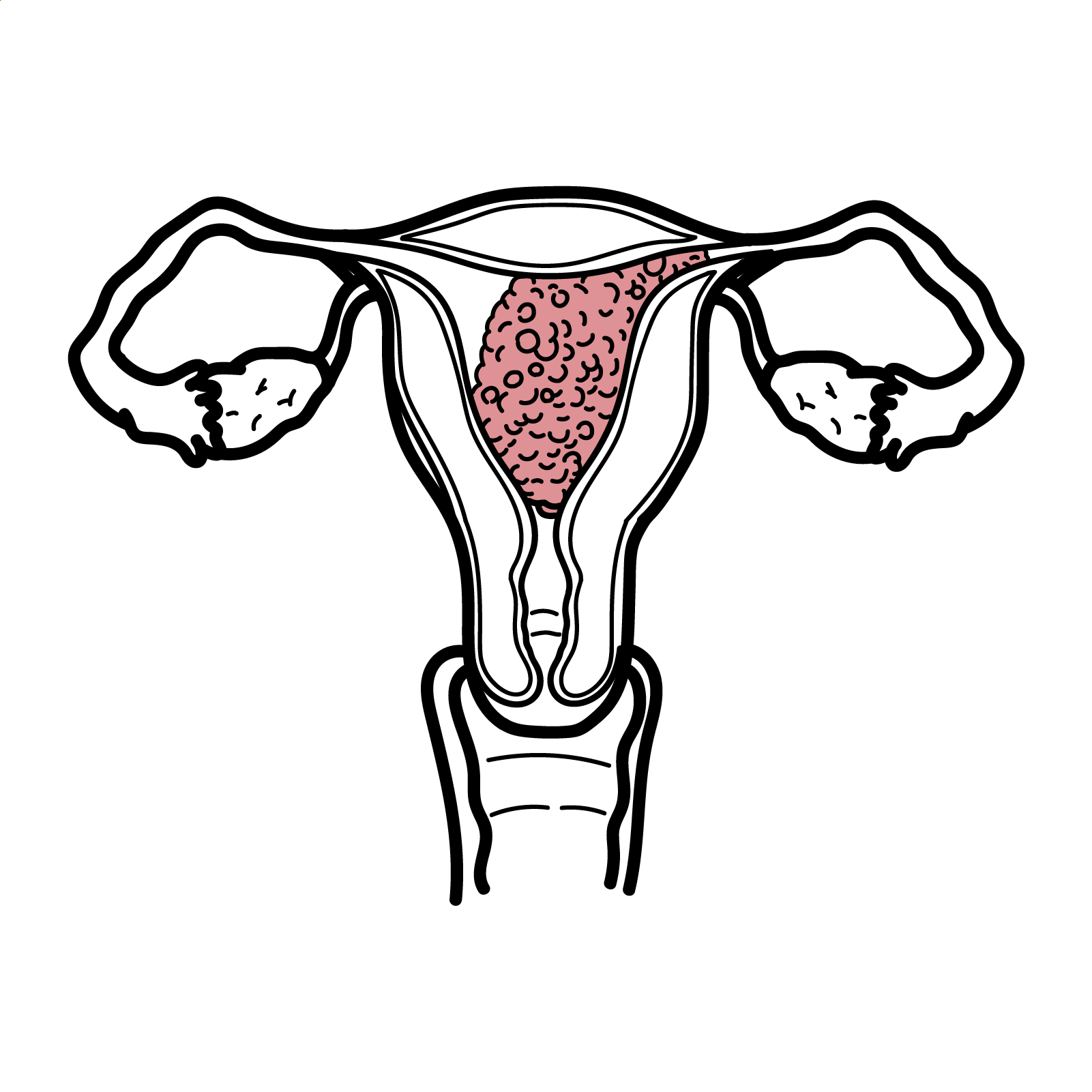
Endometrial Carcinoma: An epithelial malignancy of the uterine corpus mucosa, usually an adenocarcinoma.
Endometrial Hyperplasia: Characterised by proliferation of endometrial glands resulting in a greater gland-to-stroma ratio than is observed in normal endometrium
Endometrial Sampling (biopsy): A thin catheter is introduced through the cervix into the uterine cavity under some suction to aspirate endometrial cells.
Endometrial polyps: A growth of endometrial glands and stroma, which projects into the uterine cavity, usually on a stalk; it can cause postmenopausal bleeding.
Atrophic Endometrium: The most common cause of postmenopausal bleeding is friable tissue of the endometrium or vagina due to low estrogen levels.
Endometrial Stripe: Transvaginal sonographic assessment of the endometrial thickness; a thickness greater than 5 mm is abnormal in a postmenopausal woman.
Endometrial carcinoma is the most common female genital tract malignancy.
Epidemiology
- Most common lower gyaenocological cancer
- Most common in postmenopausal women
Atiology & Risk Factors
Aetiology
- Endometrial hyperplasia
- Unopposed endogenous/exogenous oestrogen
- Familial cancer syndromes (family history, Lynch syndrome, Cowden’s syndrome)
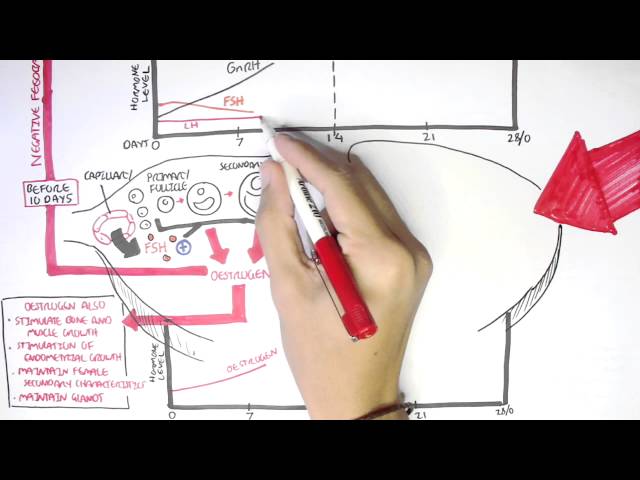
Endometrial malignancy typically developed from unopposed oestrogen. Progesterone stabilises the endometrium.
| Increased risk of endometrial cancer | Protective Factors |
| Early Menarche | Parity (high progesterone in pregnancy) |
| Post-menopausal women | Combined Oral Contraceptive Pill |
| Obestiy, Hypertension, Diabetes | |
| Endometrial hyperplasia | |
| Tamoxifen use | |
| Unopposed endogenous/exogenous oestrogen | |
| Family history of endometrial cancer | |
| Family history of ovarian and breast cancer | |
| Lynch syndrome | |
| Radiotherapy |
Endometrial carcinoma must be ruled out in any patient with postmenopausal bleeding.
Pathophysiology
Epithelial tumours (endometrial carcinoma) is the most common type of endometrial carcinoma, found in up to 90%.
Clinical Manifestation
Abnormal uterine bleeding in postmenopausal women is the cardinal symptom of endometrial cancer. Occasionally, women with no abnormal uterine bleeding present with abnormal findings on cervical cytology. The clinical presentations of the following age group need prompt evaluation to rule out endometrial cancer
- Postmenopausal women – Any bleeding
- Premenopausal (>45yo) – Abnormal uterine bleeding including intermenstrual bleeding , frequent, heavy or prolonged bleeds.
- Younger than 45yo – Persistent abnormal uterine bleeding with risk factors or failed management of the bleeding
Endometrial sampling required for women >45yo with abnormal menstrual symptoms.
Clinical Examination
- Uterine mass
- Fixed uterus or adnexal mass indicating extra-uterine disease
↑ Vaginal discharge due to infection of the uterus (Pyometra) in post-menopasual women is associated with carcinoma in 50% of cases.
Diagnosis
| Common Causes of vaginal bleeding in Postmenopausal women | |
| Causes | Definition |
| Endometrial Polyps | Hyperplastic overgrowths of endometrial glands and stroma that form a projection from the surface of the endometrium |
| Endometrial hyperplasia | Thickening if endometrial lining >4mm in post menopausal women. Increases risk of cancer. Compared with proliferative endometrium, there is an increase in the endometrial gland to stroma ratio. Endometrial hyperplasia virtually always results from chronic estrogen stimulation unopposed by the counterbalancing effects of progesterone |
| Leiomyomas (Uterine Fibroids) | Bengin, smooth muscle tumours, usually of the uterus |
| Adenomyosis | Refers to a disorder in which endometrial glands and stroma are present within the uterine musculature. The ectopic endometrial tissue appears to induce hypertrophy and hyperplasia of the surrounding myometrium, which results in a diffusely enlarged uterus |
| Atrophic vaginitis | Menopausal defiiency of estrogen resulting in thinning of vaginal epithelium resulting in increased risk of infection/inflammation and subsequent bleeding |
| Atrophic endometriosis | Endometrial thinning <4mm and inflammation that occurs as a result of esotrogen deficiency. May result in spotting or even bleeding more so in hypertensive women. |
| Hormonal therapy | |
| Anticoagulant therapy | |
| Pelvic Inflammatory Disease | Refers to acute and subclinical infection of the upper genital tract in women, involving any or all of the uterus, fallopian tubes, and ovaries; this is often accompanied by involvement of the neighboring pelvic organs. It results in endometritis, salpingitis, oophoritis, peritonitis, perihepatitis,and/or tubo-ovarian abscess. |
| CarcinomaEndometrial Adenocarcinoma (common >45 year old)Fallopian tube cancer and ovarian cancerCervical and vaginal cancer | Endometrial carcinoma is the main differential to rule out in postmenopausal women who presents with vaginal bleeding, as this accounts for 10% of cases. |
Investigations
- FBC
- Serum bHCG
- Urine bHCG
- Coagulation studies
- Pelvic Ultrasound (sonography) is first line
- Transvaginal ultrasound
- Endometrial sampling (biopsy)
- Hysteroscopy and D&C if biopsy is not possible
- Pap smear – Primarily used to screen for cervical dysplasia. It is not a screening test for endometrial cancer
Persistent postmenopausal bleeding warrants further investigation (such as hysteroscopy) even after a normal endometrial sampling.
Diagnosis Endometrial carcinoma is a histologic diagnosis made based upon the results of evaluation of an endometrial biopsy, curettage sample, or hysterectomy specimen.
Staging
| International Federation of Gynecology and Obstetrics (FIGO) staging of uterine cancer (2009) | |
| Stage | Description |
| I | Tumour invades cervical stroma, but does not extend beyond the uterus |
| II | Tumour invades cervical stroma, but does not extend beyond the uterus |
| III | Local and regional spread of the tumour |
| IV | Tumour invades the bladder and/or bowel mucosa and/or distant metastases |
Treatment
Management Endometrial cancer is treated by surgery, radiotherapy, chemotherapy, or, commonly, a combination of these therapies, with the goal of maximising the chance of cure, with minimal morbidity.
Hyperplasia is treated with progesterone (oral contraceptive) to stabilize the endometrium.
Surgery
- Staging
- Treating: Standard surgery requires a total hysterectomy, bilateral salpingo-oophorectomy, and node dissection.
Hormonal therapy
- High dose progesterone
Palliative radiotherapy
- EBRT given at lower dose and in few fractions to control local symptoms
Tumour biomarker status PTEN, Mismatch-repair genes, p53 and HER-2.
Complications & Prognosis
- Bladder instability following surgery
- Radiotherapy induced vaginal stenosis/atrophy
- Radiotherapy induced bowel or bladder distulae
- Sexual dysfunction following treatment
- Metastatic disease
- Lymphoedema
- Chemotherapy associated toxicity
Most recurrences of endometrial cancer occur within 2 years.
Prognosis The 5-year survival rate for all types and grades of endometrial adenocarcinoma, following treatment, is:
- 75% to 95% for stage I
- 70% for stage II
- 50% to 60% for stage III
- 5% to 15% for stage IV








Members only discussions coming soon…