

Cervical Cancer

Overview
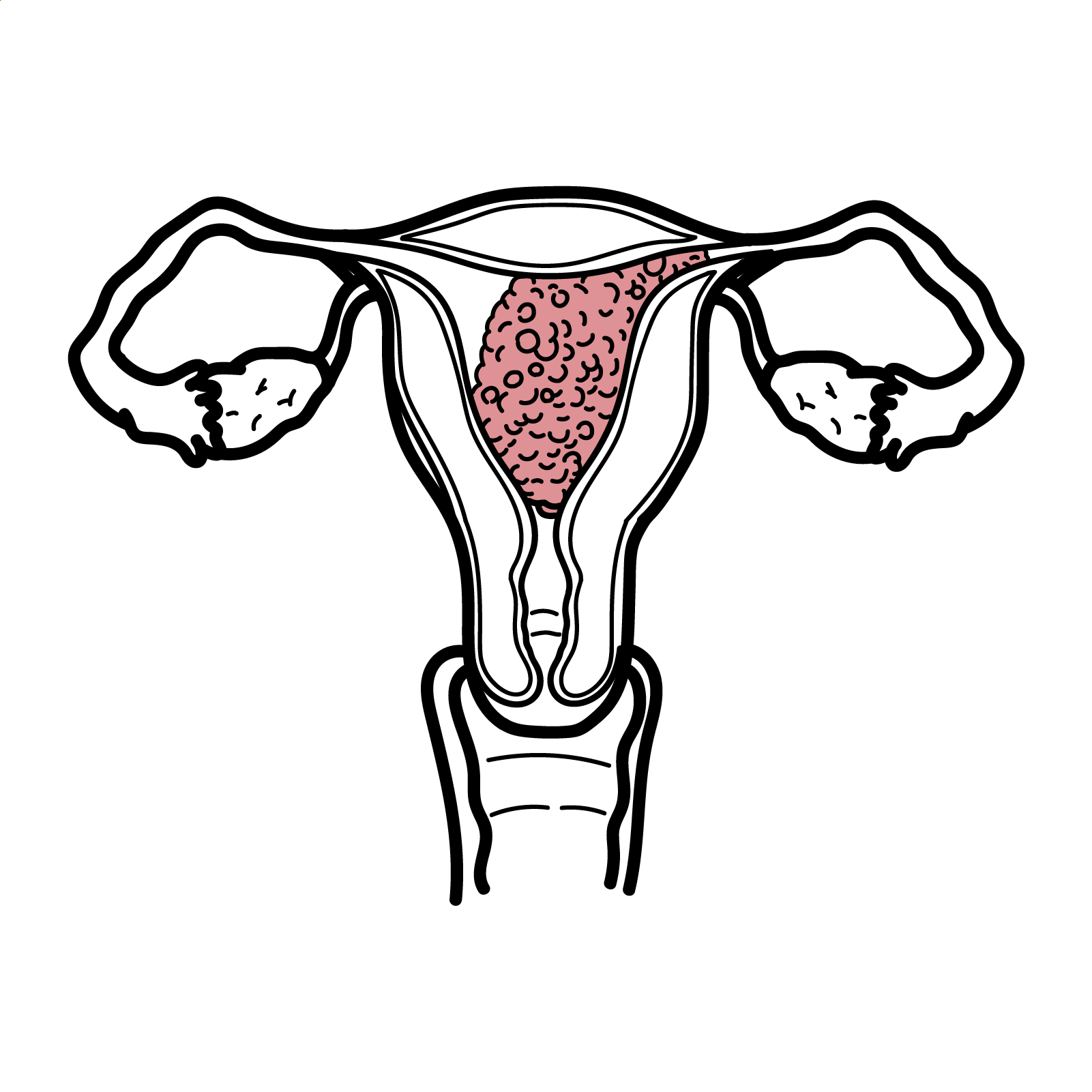
Cervical cancer is an HPV-related malignancy of the uterine cervical mucosa. Most cervical tumours contain HPV DNA (99.7%) . There are many variants of HPV, HPV-16 and 18 are the 2 most common high-risk types. Cervical cancer is proceeded by an idenifiable precursor lesion (cervical intraepithelial neoplasia (CIN1)) that may progress to invasive cancer. CIN can be easily detected by an inexpensive and noninvasive screening test (Pap smear). Pap smears has been hailed as one of the most successful preventative medical strategies. Cervical cancer is the second most common cancer in women.
Definition
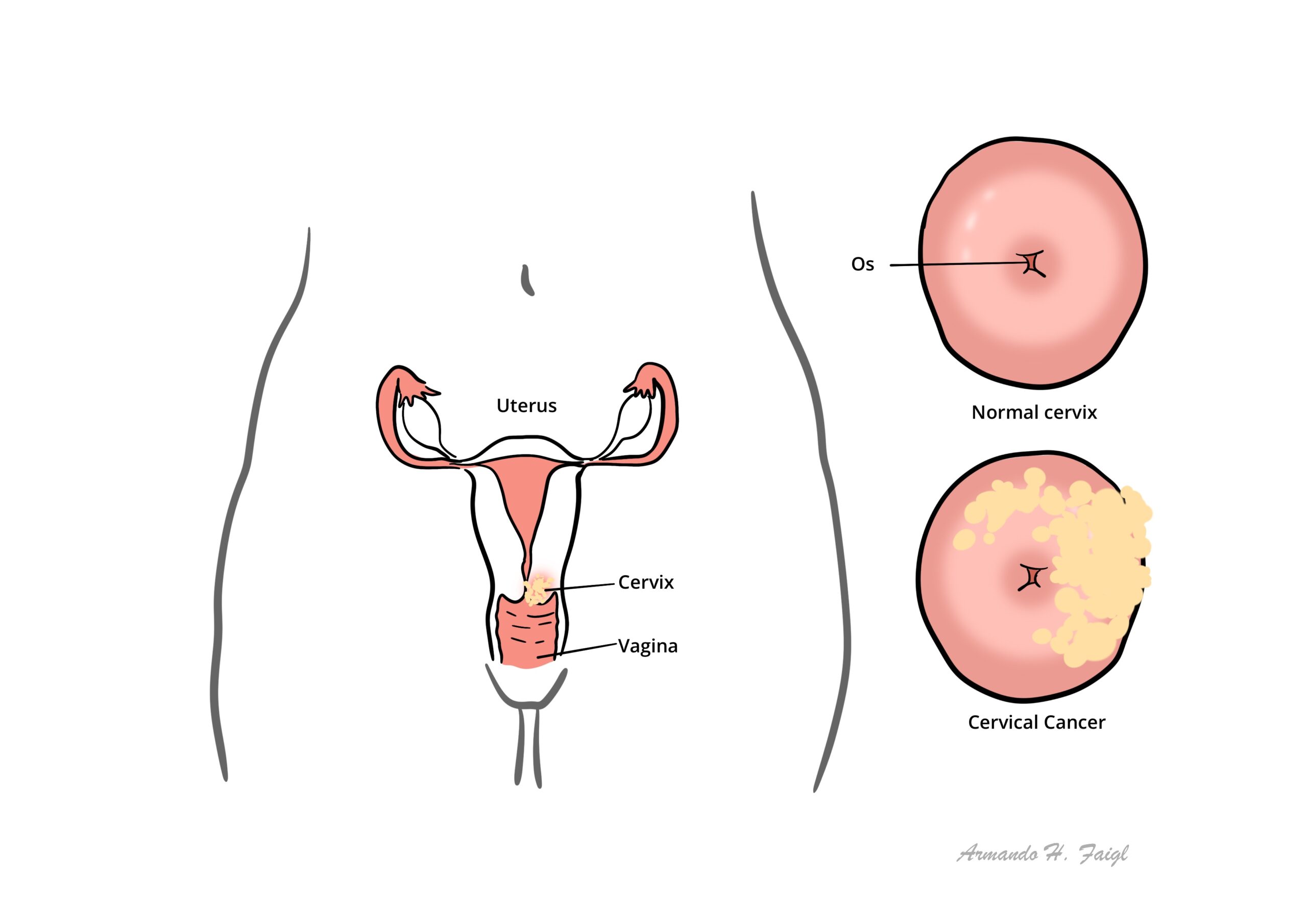
Cervix: Cylinder-shaped neck of tissue that connects the vagina and uterus.
Transitional zone of the cervix: Dynamic entity formed during puberty and, histologically, is the area where the glandular epithelium is being replaced by squamous epithelium
Squamo–Columnar Junction (SCJ): Point at which columnar and squamous epithelium meet at the cervix.
Pap Smear: Screening tool where samples cells are taken from the junction of the ectocervix and endocervix (the transformation zone or squamocolumnar junction, where 90% of cervicalneoplasias originate) to identify pre-malignant or malignant lesions
High Risk HPV: Also known as oncogenic HPV types (most commonly 16 and 18) are the most common causes of invasive cervical cancers and 50% of high grade lesions
LLETZ: Large loop excision of the transformation zone is a procedure to remove cervical tissue for examination and to treat some precancerous changes of the cervix.
Epidemiology
- Most common gynaecological malignancy in young women
Pathology
Cytology (Pap smear) – screening
- Negative
- Abnormal – unknown (ASCUS)
- LSIL
- HSIL
- Cancer
- CIN1 (correlated with LSIL)
- CIN2 (HSIL)
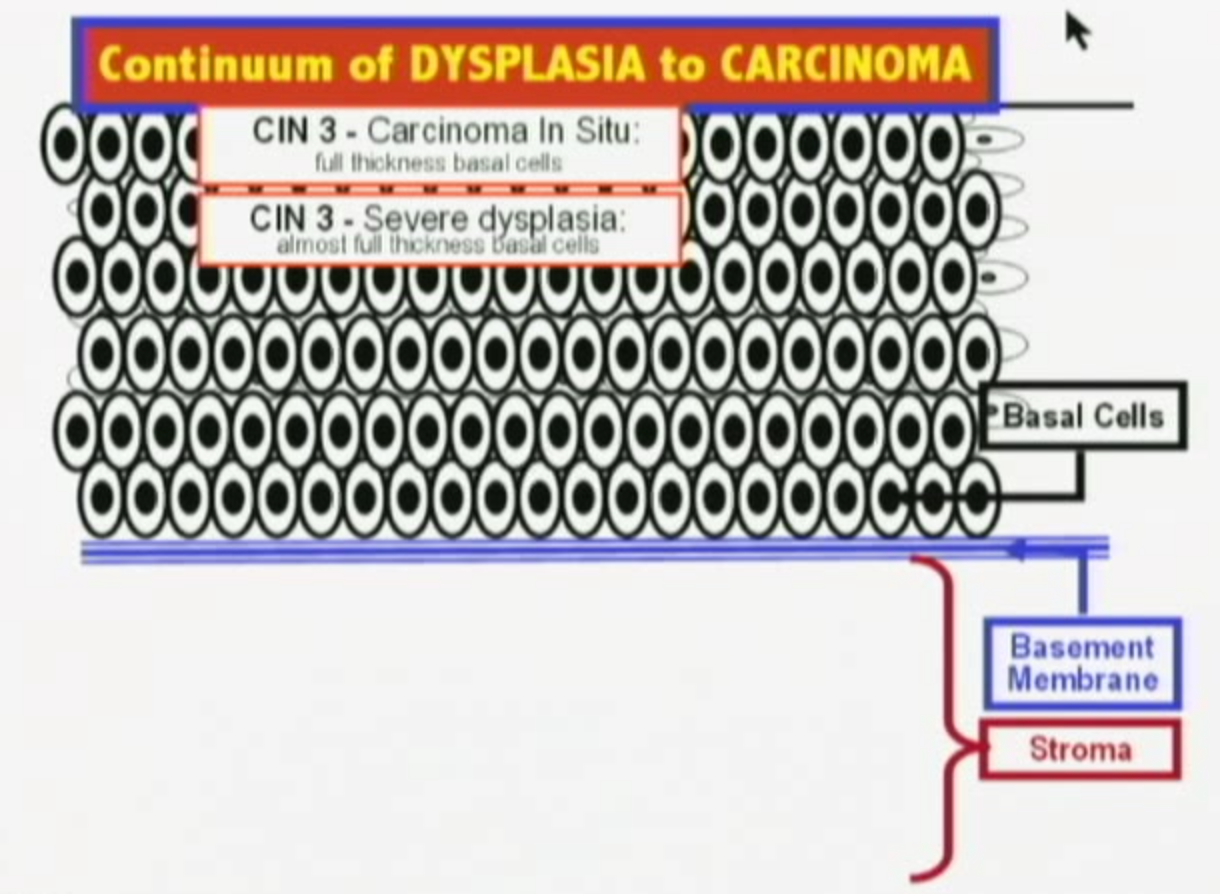
- CIN3 (HSIL)
- Cancer
- Squamous cell carcinoma (85%) caused by HPV 16
- Adenocarcinoma (10%) caused by HPV 18
Rarer:
- Neuroendocrine tumour
- Clear cell carcinoma
- Glassy carcinoma
- Lymphoma o cervix
Risk Factors
- Early age of coitus
- Sexually transmitted diseases
- Early childbearing
- Low socioeconomic status
- Human papillomavirus
- HIV infection (Immunosupression)
- Cigarette smoking
- Multiple sexual partners
Pathophysiology
There are approximately 200 different types of HPV, which are classified according to DNA sequence. Between 40–50 HPV types specifically infect the anogenital area and, less commonly, the oro-pharyngeal area. These genital HPV types are divided into ‘low risk’ and ‘high risk’ according to their association with, and ability to cause, anogenital cancer.
- Low risk: HPV 6 and 11 cause genital warts
- High risk or oncogenic HPV types (15types): HPV 16 and 18 are the two most common causes of invasive cervical cancers and 50% of high grade lesions
Development of cervical cancer
There are four main steps for the development of cervical cancer:
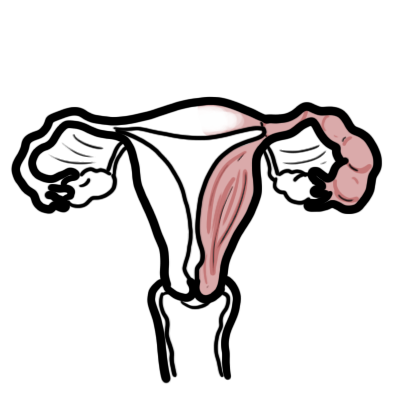
- Infection of the metaplastic epithelium at the cervical transformation zone (the squamo-columnar junction) with a high risk or oncogenic type of HPV (16 or 18)
- HPV infect basal cells in this area
- Persistent infection with an oncogenic HPV type
- Progression of persistently infected epithelium to pre-cancerous changes (HSILs), typically taking 1–15 years to become established
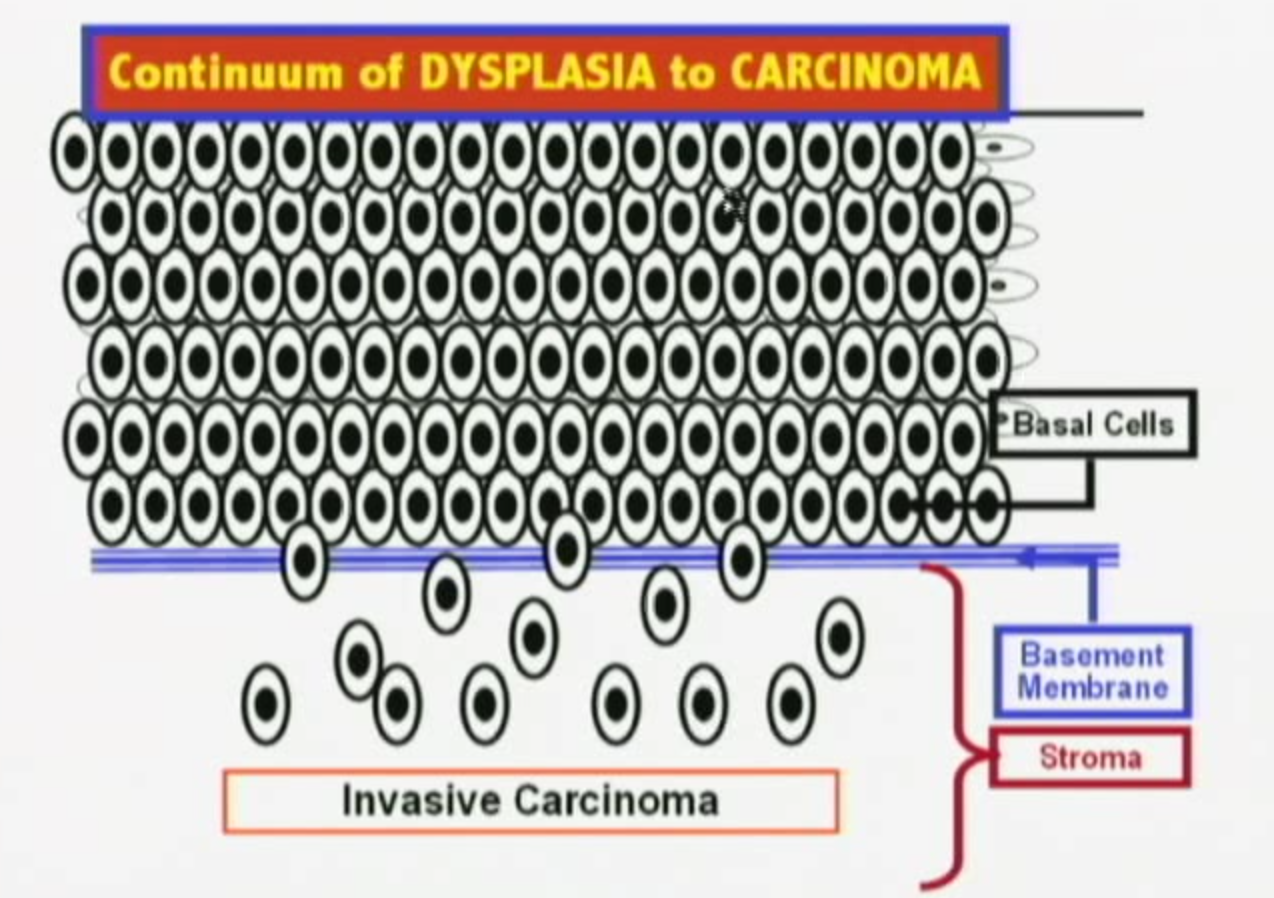
- Invasion through the basement membrane of the epithelium. Invasive cervical cancer develops over many years. Rapid onset cancers can occur, but they are very rare.
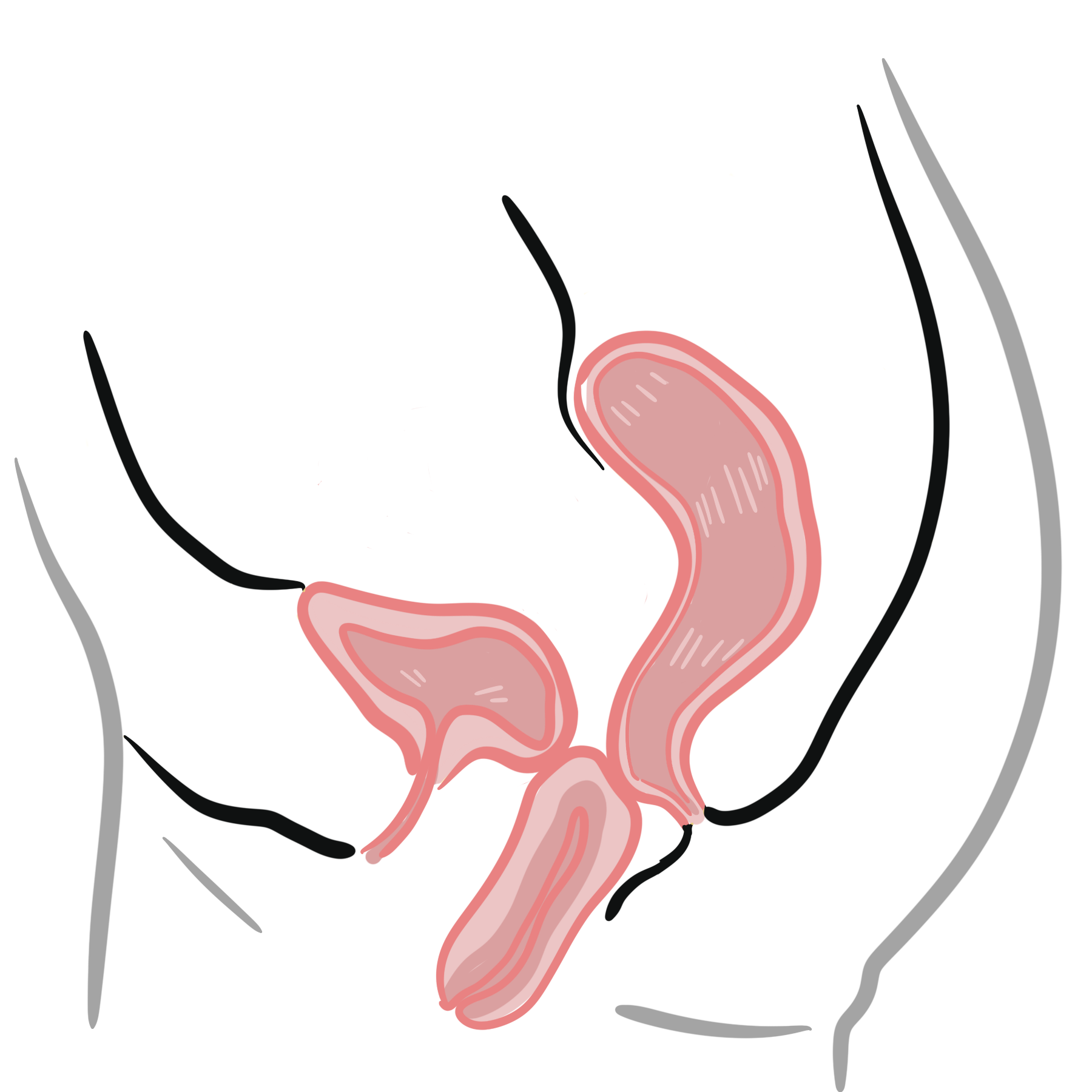
ROUTES OF SPREAD — Cervical cancer can spread by direct extension or by lymphatic or hematogenous dissemination.
Clinical Manifestation
Early stage disease is frequently asymptomatic. Pre-invasive lesions are often found only after abnormal routine screening Pap smear. Abnormal vaginal bleeding is the most common presenting symptom of invasive cervical cancer, and in sexually active women, postcoital spotting is common. Mean age of developing cervical cancer is 50yo.
- Abnormal vaginal bleeding
- Postmenopausal bleeding (1% of cases)
- Postcoital bleeding
- Mucoid or purulent vaginal discharge
- Pelvic pain, dyspareunia
- Cervical mass
Flank tenderness or leg swelling indicate advanced cervical cancer.
Diagnosis
- Cervicitis (STD)
- Nabothian cyst (mucus filled cyst)
- Endometriosis
- Cervical polyp
- Cervical Fibroid
- Cervical Eversion
- Conyloma accuminata (caused by HPV 6, 11)
Investigations
Investigations A cervical biopsy and not pap smear is the best diagnostic test to evaluate a cervical mass. A Pap smear is a screening test and appropriate for a woman with a normal- appearing cervix.
- FBC
- EUC
- LFT
- CT abdomen and pelvis (staging and preoperative assessment)
- MRI – pelvis
- HPV DNA typing
- Colpscopy
Diagnosis Cervical biopsy is the most important investigation in diagnosing cervical cancer. Cervical cancer is a clinically staged disease
Cervical cancer is a clinically staged disease.
Compare pap smear and biopsy. They should correlate with each other. If biopsy not significant but pap smear significant further investigation is warranted (cone biopsy).
Staging
| FIGO (International Federation of Gynecology and Obstetrics) staging of cervical cancer | |
| Stage | Description |
| I | Confined to the cervix (uterine spread not evaluated) |
| II | Cancer invades beyond the cervix but not to the pelvic sidewall, or the distal third of the vagina |
| III | Tumour affixed to pelvic sidewall, or involving the lower third of the vagina, or is associated with a non-functioning kidney or hydronephrosis |
| IV | Carcinoma has extended out of the pelvis, involving the bladder, or rectum. |
Treatment
Overview
- Observations (repeat pap smear)
- Ablation (Cyrotherapy, Laser)
- Excision (LEETZ)
- Hysterectomy
| MANAGEMENT OVERVIEW | ||||
| Biopsy | Observation | Ablation | Excision | Hysterectomy |
| CIN1 | + | + | + | |
| CIN2/CIN3 | + | + | +/- | |
| Cancer | + | |||
Microinvasive Disease (Stage I)
- Local excision +/- lymphadenectomy
Early Stage Disease (Stage I-II)
- Radical hysterectomy with lymphadenectomy is preferred to chemoradiation for patients with non-bulky tumours
- Fertility sparing surgery – Radical trachelectomy (excision of the cervix) with lymphadenectomy (excision of the cervix)
Locally Advanced Disease (Stage II-IV)
- Chemoradiotherapy is the standard of care for locally advanced and early stage cancers with poor prognostic factors
Metastatic disease (Stage IV)
- Chemotherapy is palliative only in patients with recurrent or metastatic disease
Complications & Prognosis
- Surgery Complications (Hysterectomy and lymphadectomy)
- Bleeding
- Bladder instability
- DVT/PE
- Lymphoedema
- Lymphocysts
- Ureteric fistula
- Radiotherapy complications
- Vaginal stenosis/atrophy
- Bowel or bladder Fistulae
- Sexual dysfunction following treatment
- Metastatic disease
- Chemotherapy associated toxicity
Most recurrences of endometrial cancer occur within 2 years.
Prognosis The 5-year survival depends on the stage of the tumour:
- Stage IA1 – 100%
- Stage IB2-IIB – 50% to 70%
- Stage III – 30% to 50%
- Stage IV – 5% to 15%.
Prevention
Vaccination
Vaccination against human papillomavirus (HPV) is recommended due to the link between cervical HPV infection and the development of cervical dysplasia.
Pap smear
Cervical cancer screening (Pap Smear) is very effective. It has been associated with a 70% reduction in cervical cancer mortality in developed countries. The Pap smear samples cells from the junction of the ectocervix and endocervix (the transformation zone or squamocolumnar junction, where 90% of cervicalneoplasias originate) to identify pre-malignant or malignant lesions
In Australia pap test screening is recommended every 2 years for women who have ever had sex and have an intact cervix, commencing from age 18–20 years (or up to 2 years after first having sexual intercourse, whichever is later).
Results can be as follows:
- Normal (negative for intraepithelial lesion or malignancy)
- Epithelial cell abnormality
- Squamous cell
- Atypical squamous cells of undetermined significance
- Atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion (ASC-H)
- Low-grade squamous intra-epithelial lesion (LSIL); consistent with HPV infection and possible histological finding of cervical intra-epithelial neoplasia (CIN)-1
- High-grade squamous intra-epithelial lesion (HSIL); HSIL cytology suggests moderate dysplasia, cvarcinoma in situ, or CIN-II and -III on biopsy
- Squamous cell carcinoma
- Glandular cell
- Atypical glandular cells
- Endocervical adenocarcinoma in situ (ACIS)
- Adenocarcinoma
- Other
- Adenosquamous
- Adenoid cystic carcinoma
- Neuroendocrine
- Squamous cell
The most common histologic types of cervical cancer are squamous cell (85% of cervical cancers) and adenocarcinoma (10%).
Adenosquamous tumors exhibit both glandular and squamous differentiation. They may be associated with a poorer outcome than squamous cell cancers or adenocarcinomas.
References
BestPractice
UpToDate
Petignat, P., & Roy, R. (2007). Diagnosis and Management of cervical cancer. The BMJ. 335 (765).
Stella, H. (2014). HPV testing in the National Cervical Screening Program. RACGP. 42 (7). 463-466.







Members only discussions coming soon…