

Genital Prolapse
Overview
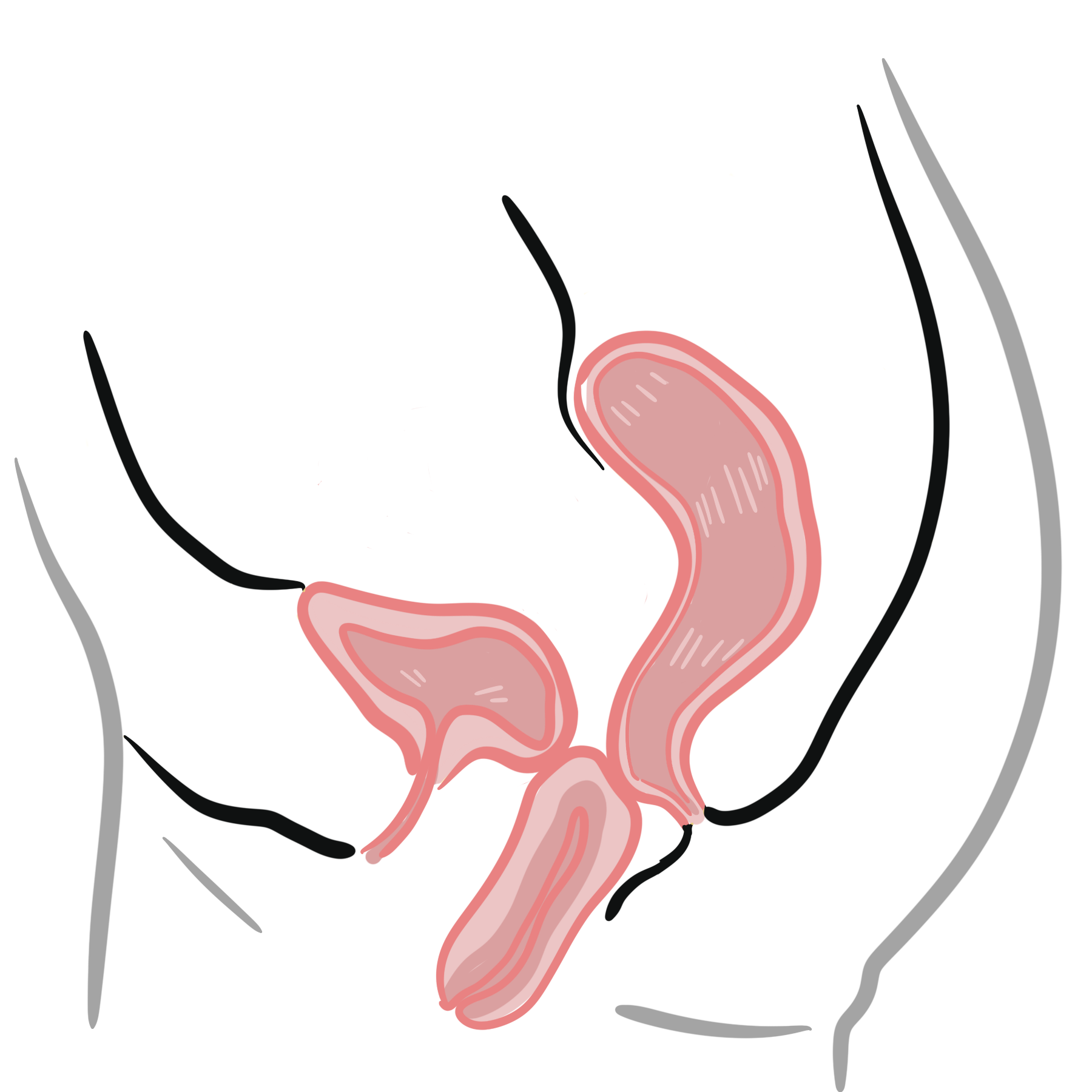
Genital prolapse, or Pelvic Organ Prolapse (POP), is the symptomatic anatomical descent of one or more pelvic structures—including the anterior vaginal wall, posterior vaginal wall, uterus, or vaginal vault following a hysterectomy. It occurs due to a progressive loss of structural support provided by the pelvic floor muscles, endopelvic fascia, and associated ligamentous attachments. This breakdown allows pelvic viscera to herniate into or beyond the vaginal introitus, resulting in mechanical displacement and functional impairment of the lower urinary, gastrointestinal, and reproductive tracts.
Epidemiologically, pelvic organ prolapse is a widespread gynaecological condition affecting up to 50% of parous women over the age of 50. The prevalence increases significantly with age, multiparity, and menopausal status. Although prolapse is rarely life-threatening, it causes substantial morbidity, leading to chronic physical discomfort, urinary and fecal dysfunction, impaired sexual health, and reduced quality of life. The lifetime risk of a woman requiring surgical intervention for pelvic organ prolapse or urinary incontinence by age 80 is estimated at 10–20%.
Definition
Pelvic Organ Prolapse Quantitation (POP-Q): An objective, site-specific system used to describe and stage pelvic organ prolapse relative to the hymenal ring.
Cystocele: Herniation of the bladder through the weakened anterior vaginal wall.
Rectocele: Herniation of the anterior rectal wall through the posterior vaginal wall.
Enterocele: Herniation of the rectouterine pouch (Pouch of Douglas), containing small bowel loops, into the upper posterior vaginal wall.
Uterine Prolapse: Downward displacement of the uterus and cervix into the vaginal canal.
Procidentia: Severe, complete prolapse in which the entire uterus and vagina evert outside the hymenal ring.
Vaginal Vault Prolapse: Descent of the top of the vagina (surgical cuff) following a hysterectomy.
Anatomy
Anatomy – Genital Support (De Lancey – 3 level of support)
- Uterosacral and cardinal ligaments – support the uterus and vaginal vault
- Pelvic Floor Muscles
- Levator Ani
- Illiococcygeus
- Anteversion of the uterus
Organs that support
- Musculature
- Levator ani
- Ligaments and connective tissue
- Endopelvic fascia
- Vaginal wall
Classification
Compartmental Classification
- Anterior Compartment: Cystocele, urethrocele.
- Apical Compartment: Uterine prolapse, vaginal vault prolapse (post-hysterectomy), enterocele.
- Posterior Compartment: Rectocele.
POP-Q Staging System
- Stage 0: No prolapse demonstrated; anatomical points remain at baseline.
- Stage I: Most distal portion of the prolapse is > 1 cm above the hymen.
- Stage II: Most distal portion of the prolapse is within 1 cm above or below the hymen (between -1 cm and +1 cm).
- Stage III: Most distal portion of the prolapse is > 1 cm below the hymen, but descends no further than 2 cm less than Total Vaginal Length (TVL).
- Stage IV: Complete eversion of the total length of the lower genital tract (procidentia).
The hymenal ring serves as the fixed anatomical point of origin (0 cm) in the POP-Q system to measure and stage prolapse severity.
Risk Factors
Obstetric Factors (Primary Risk Factor)
- Multiparity & Vaginal Delivery: Causes direct mechanical tearing, stretching, and denervation of the levator ani muscle complex and endopelvic fascia.
- Instrumental Delivery: Forceps or vacuum-assisted delivery increases pelvic floor trauma.
- Prolonged Second Stage of Labor & Fetal Macrosomia.
Age & Hormonal Factors
- Advanced Age & Menopause: Estrogen deficiency causes atrophy, reduced collagen synthesis, and loss of tissue elasticity in the endopelvic fascia.
Chronically Elevated Intra-Abdominal Pressure
- Obesity & Chronic Constipation / Straining.
- Chronic Cough: Secondary to COPD, asthma, or smoking.
- Occupational Straining: Heavy manual lifting.
Connective Tissue & Genetic Factors
- Heritable Connective Tissue Disorders: Ehlers-Danlos Syndrome, Marfan Syndrome.
- Family History: First-degree relative with pelvic organ prolapse.
Iatrogenic Factors
- Prior Pelvic Surgery: Hysterectomy or pelvic floor reconstruction disturbing natural anatomical support vectors.
Vaginal childbirth is the single most important modifiable or preventable risk factor for the development of pelvic organ prolapse in later life.
Pathophysiology
- Structural Support Failures (DeLancey Levels):
- Level 1 (Suspension): Uterosacral and cardinal ligament complex suspending the apex of the vagina and cervix to the sacrum and lateral pelvic walls. Failure causes apical prolapse (uterine or vault).
- Level 2 (Attachment): Pubocervical fascia laterally attaching the anterior vaginal wall to the arcus tendineus fasciae pelvis, and rectovaginal fascia attaching the posterior wall. Failure causes cystocele or rectocele.
- Level 3 (Fusion): Distal vaginal fusion to the perineal body and levator ani muscles. Failure causes perineal hypermobility and distal vaginal descent.
- Levator Ani Dysfunction: Chronic levator ani muscle injury or denervation impairs its baseline resting tone, widening the urogenital hiatus and forcing the endopelvic fascia to bear the full force of intra-abdominal pressure.
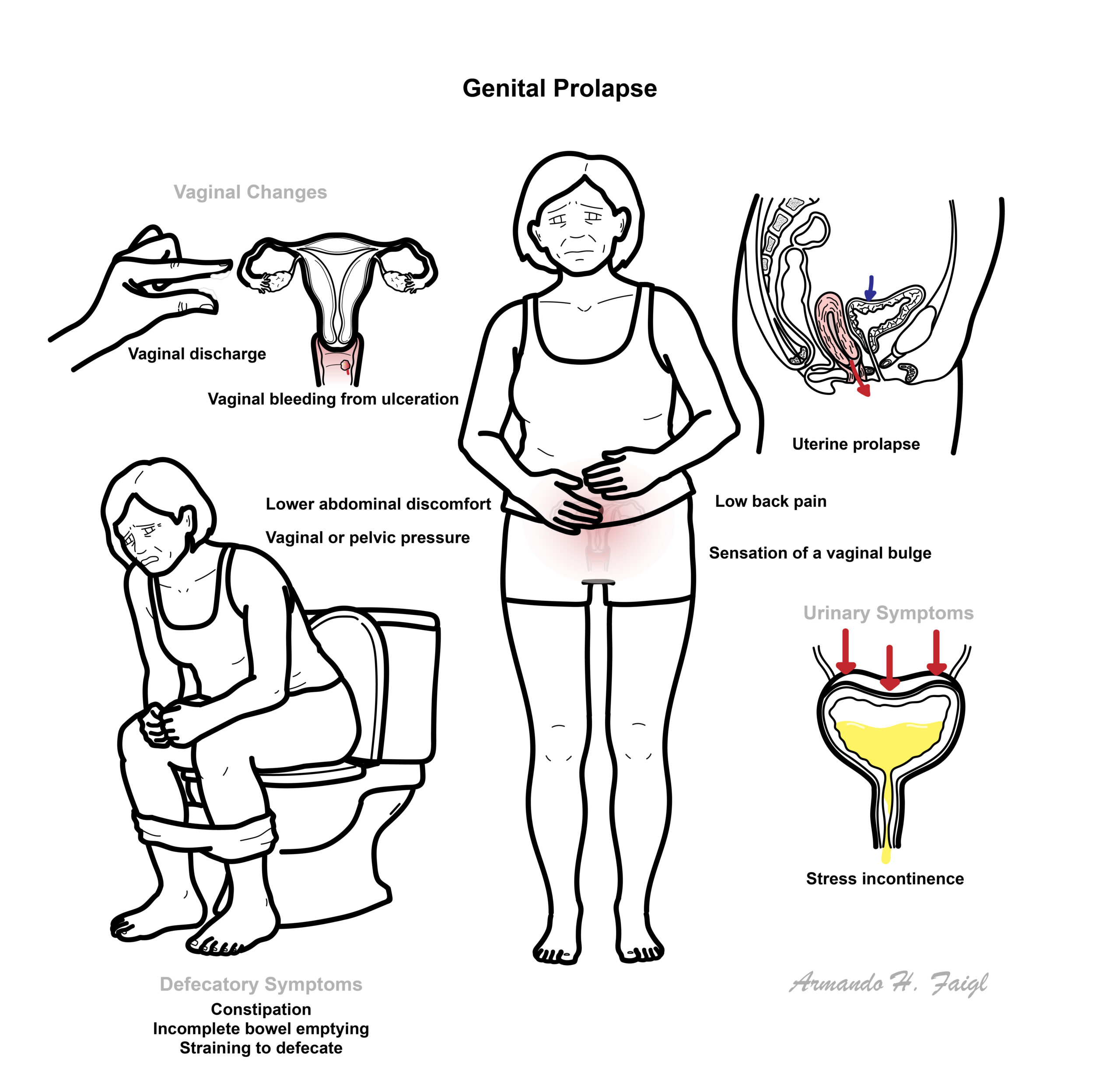
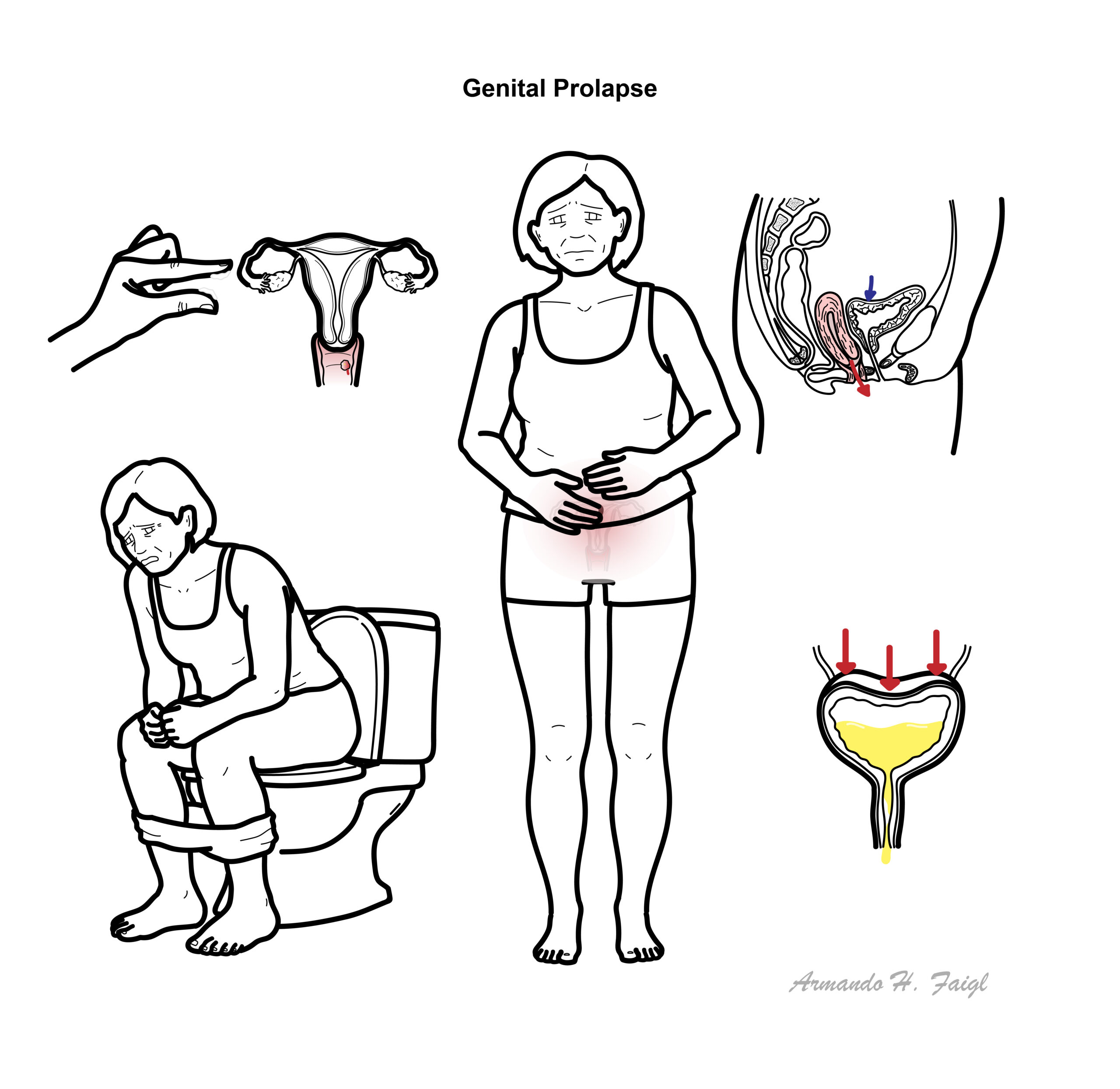
Clinical Manifestations
Local & Mechanical Symptoms
- Vaginal Bulge / Fullness: Sensation of “something coming down” or a visible mass bulging at or beyond the vaginal introitus (most specific symptom).
- Pelvic Pressure / Heaviness: Dull lower backache or pelvic drag that worsens towards the end of the day or after prolonged standing.
- Mucosal Ulceration & Bleeding: Friction drying and excoriation of exposed vaginal mucosa against clothing causing discharge or spotting.
Urinary Symptoms (Associated with Anterior Prolapse)
- Urinary Hesitancy & Weak Stream: Mechanical kinking of the urethra by a large cystocele.
- Incomplete Bladder Emptying: High post-void residual volume.
- Manual Splinting: Patient needs to reduce the anterior prolapse manually (“pushing the bulge up”) to initiate or complete urination.
- Overactive Bladder & Stress Incontinence: Frequency, urgency, or co-existing stress urinary incontinence.
Bowel Symptoms (Associated with Posterior Prolapse)
- Constipation & Incomplete Evacuation: Stool trapping within a rectocele pocket.
- Manual Splinting for Defecation: Patient needs to press digitally against the posterior vaginal wall or perineum to evacuate stool.
- Fecal Urgency / Incontinence.
Sexual Dysfunction
- Dyspareunia & Fear of Leakage: Pain or embarrassment during intercourse due to physical obstruction.
Manual splinting (pushing the vaginal bulge back up digitally to urinate or evacuate stool) is a classic symptom of advanced anterior or posterior pelvic organ prolapse.
Diagnosis
Physical Examination (Lithotomy or Left Lateral Position)
- Visual Inspection: Examine the vulva at rest and during maximum Valsalva maneuver to identify the leading edge of the prolapse.
- Speculum Examination: Use a single-bladed Sims speculum to isolate the anterior wall, posterior wall, and apex independently during Valsalva.
- POP-Q Assessment: Objective measurement of 9 anatomical points relative to the hymen.
- Bimanual & Rectovaginal Exam: Evaluate uterine size, adnexa, and differentiate between a rectocele and enterocele (feeling impulse in rectovaginal septum during coughing).
Diagnostic Investigations
- Urinalysis & Urine Culture: Exclude urinary tract infection in patients with voiding dysfunction.
- Post-Void Residual (PVR) Volume: Bedside bladder scan to evaluate for urine retention caused by urethral kinking.
- Urodynamic Studies: Indicated if there is co-existing urinary incontinence, voiding dysfunction, or to evaluate for “masked/occult” stress urinary incontinence after manual prolapse reduction.
- Renal Ultrasound: Indicated in severe Stage 3 or 4 procidentia to rule out bilateral ureteric obstruction and hydronephrosis.
Always perform a post-void residual (PVR) scan and evaluate for hydronephrosis via renal ultrasound in patients with severe Stage 3 or 4 procidentia due to the risk of ureteric kinking and silent renal failure.
Treatment
General Management (First-Line)
- Lifestyle Modifications
- Weight loss
- Treatment of chronic cough/constipation
- Avoidance of heavy lifting
- Smoking cessation.
- Pelvic Floor Muscle Training (PFMT / Kegels)
- Supervised by a specialist physiotherapist for at least 3–6 months
- Best suited for mild-to-moderate (Stage 1–2) prolapse to prevent progression and reduce symptoms.
Mechanical Management (Pessary Therapy)
- Vaginal Pessaries (Support vs. Space-Occupying): Ring pessaries (first-line for mild/moderate) or Gellhorn/Gellhorn-type pessaries (for severe prolapse or weak pelvic floor).
- Indications: Patients who decline surgery, desire future childbearing, are medically unfit for anesthesia, or during pregnancy.
- Maintenance: Requires regular removal and cleansing every 3–6 months, along with co-prescription of topical vaginal estrogen in postmenopausal women to prevent mucosal ulceration.
Surgical Management (Symptomatic / Refractory Cases)
- Reconstructive Surgery (Anterior/Posterior Compartments):
- Anterior Colporrhaphy: Plication of pubocervical fascia for cystocele repair.
- Posterior Colporrhaphy: Plication of rectovaginal fascia for rectocele repair.
- Reconstructive Surgery (Apical Compartment):
- Vaginal Hysterectomy: Removal of uterus with apical suspension.
- Uteropexy / Sacrospinous Ligament Fixation (SSLF): Suspends the uterus or vaginal vault to the sacrospinous ligament.
- Abdominal / Laparoscopic Sacrocolpopexy: Gold standard for post-hysterectomy vaginal vault prolapse using synthetic mesh to suspend the vault to the sacral promontory.
- Obliterative Surgery:
- Colpocleisis (LeFort Colpocleisis): Surgical closure/sewing together of the vaginal walls. Reserved for elderly patients with severe prolapse who are no longer sexually active and cannot tolerate extensive reconstructive surgery.
Topical vaginal estrogen should be co-prescribed with a vaginal pessary in postmenopausal women to prevent mucosal excoriation, ulceration, and bleeding.
Complications & Prognosis
- Vaginal Mucosal Ulceration & Infection
- Obstructive Uropathy & Renal Failure: Ureteric kinking in severe procidentia leading to bilateral hydronephrosis and acute/chronic renal impairment.
- Recurrent Urinary Tract Infections
- Occult Stress Incontinence
- Pessary Complications
- Surgical recurrence occurs in up to 25–30% of patients following primary reconstructive repair, often due to persistent underlying tissue weakness or uncorrected intra-abdominal pressure factors.
References
- Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet. 2007;369(9566):1027-1038. doi:10.1016/S0140-6736(07)60462-0
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4-20. doi:10.1002/nau.20798
- Maher C, Feiner B, Baessler K, Christmann-Schmid C, Haya N, Brown J. Surgery for women with apical vaginal prolapse. Cochrane Database Syst Rev. 2016;10(10):CD012376. doi:10.1002/14651858.CD012376









Members only discussions coming soon…