Chronic compartment syndrome (also known as chronic exertional compartment syndrome or exercise induced compartment syndrome) is an exertional condition in which repetitive activity causes transiently elevated pressure within a closed myofascial compartment, leading to ischemic pain, tightness, and sometimes neurologic symptoms that predictably begin with exercise and abate with rest. It most often affects young, physically active people (runners, team-sport athletes, military recruits) and may account for a substantial proportion of exercise-related lower-leg pain; upper-limb cases occur in rowers, climbers, weightlifters, and motorcycle racers. 1,2,3,4 Risk increases with high training volumes, running gait mechanics that increase anterior compartment demand, and fascial stiffness; outcomes range from successful return to sport with gait retraining or fasciotomy to persistent or recurrent symptoms if diagnosis is delayed. 1,5,6
Definition
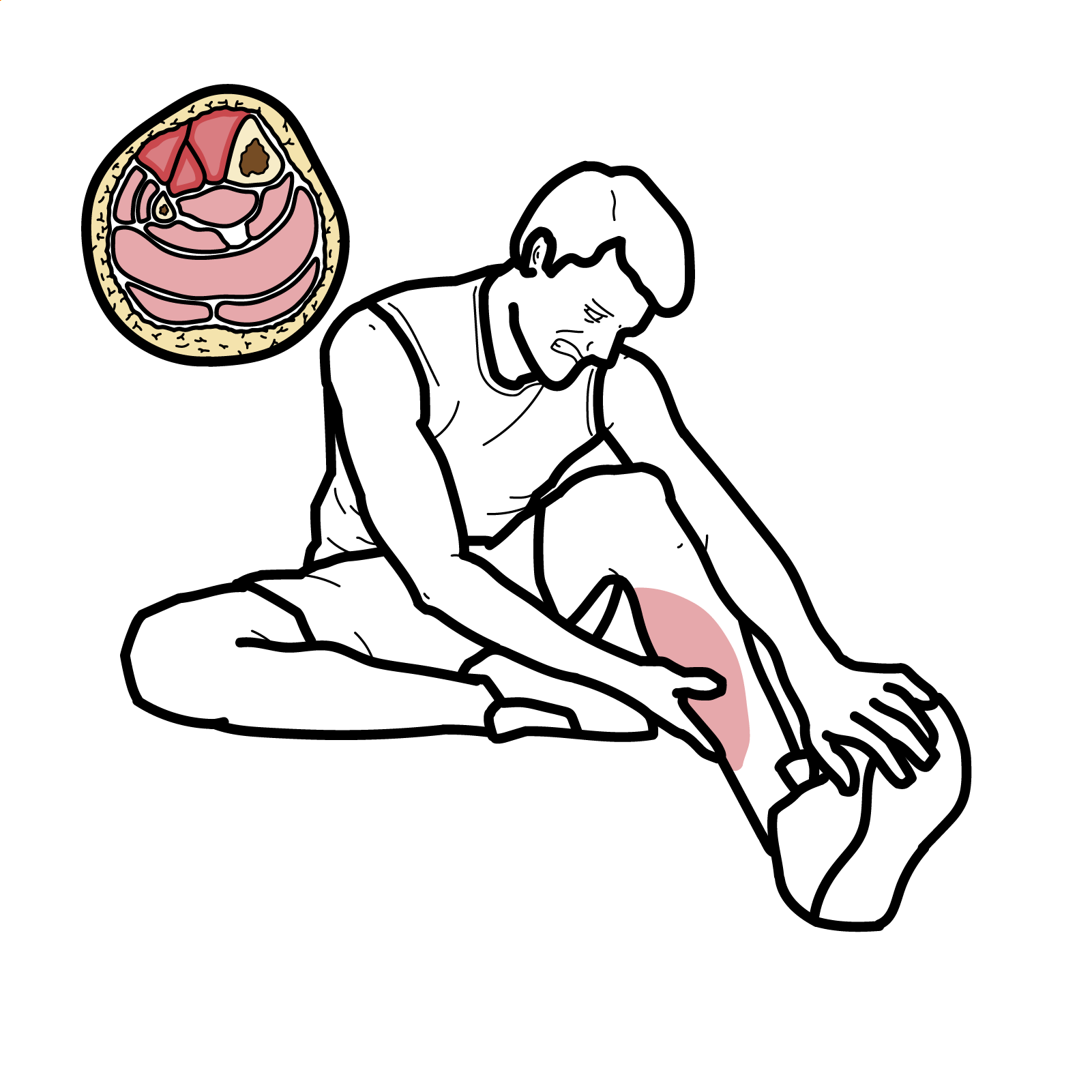
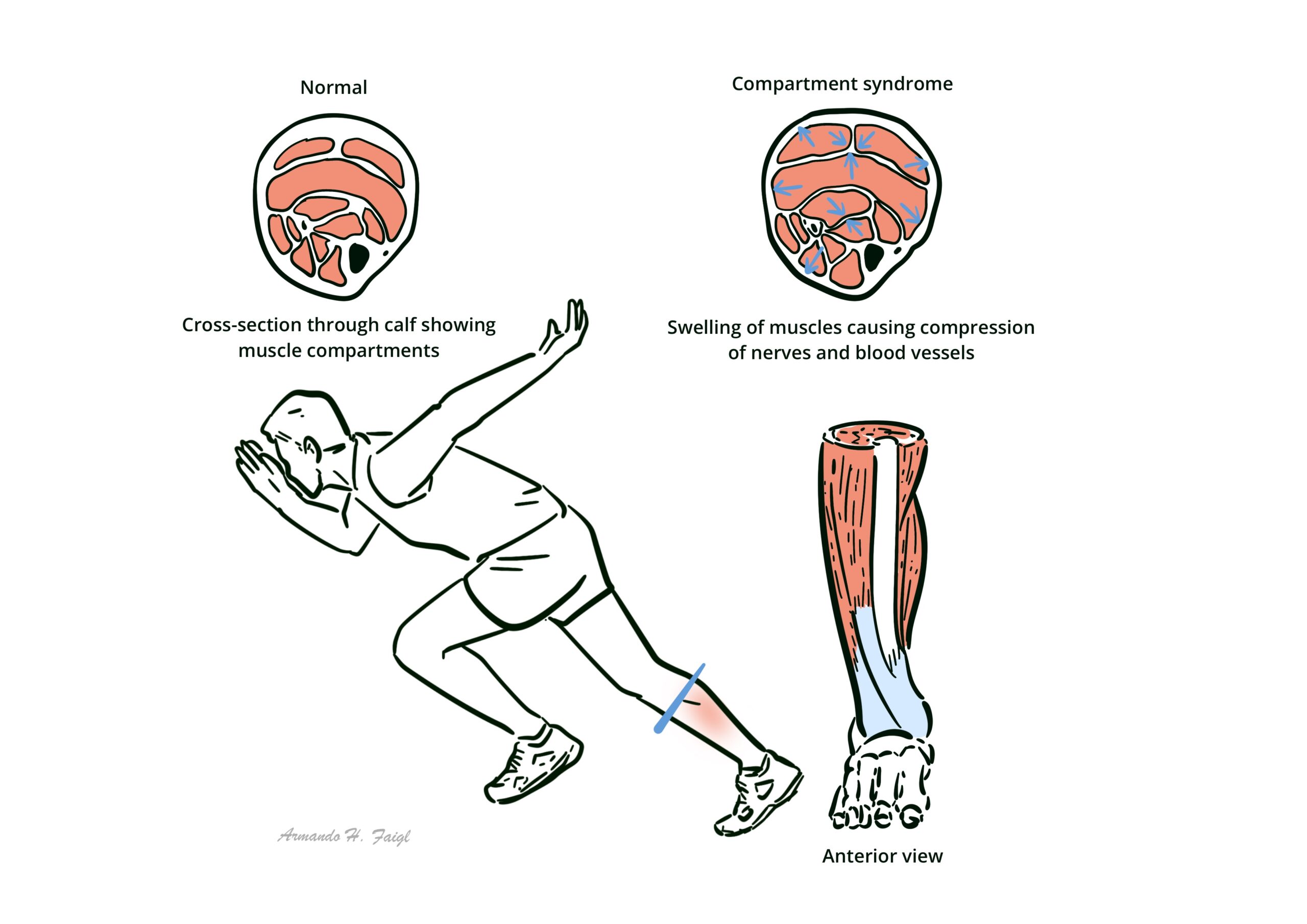
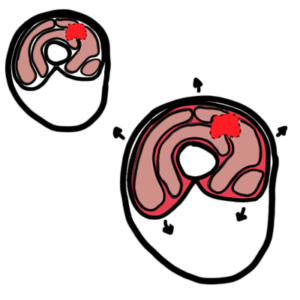
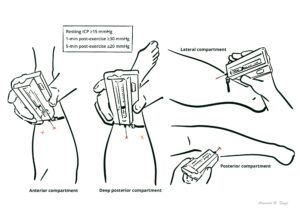
Compartment: A limb space bounded by rigid fascia containing muscle groups, nerves, and vessels. Intracompartmental pressure (ICP): Pressure within a compartment; measured with a needle/catheter manometer at rest and after exercise. Chronic exertional compartment syndrome (CECS): exertional condition in which repetitive activity causes transiently elevated pressure within a closed myofascial compartment, leading to ischemic pain, tightness, and sometimes neurologic symptoms that predictably begin with exercise and abate with rest. Fasciotomy: Surgical decompression of a compartment by incising the fascia. Ischemia: Inadequate perfusion causing exertional pain and paresthesia in CECS.
Fascial mechanics: Inelastic fascia limits radial expansion; muscle volume acutely increases with hyperemia during exercise; venous outflow depends on muscle pump and low extravascular pressure.
Emerging options: Botulinum toxin A injections may normalize ICP and relieve symptoms in small series/case reports; evidence low-quality; transient strength loss reported.
Surgical (for refractory, pressure-positive CECS or failed conservative care):
Open or endoscopic fasciotomy of involved compartments; both approaches show similar return-to-sport and satisfaction rates in comparative series.
Forearm CECS: endoscopic/mini-open fasciotomy yields high return to sport with low recurrence in small series.
Post-op rehab protocols vary; progressive running/return-to-play typically staged over weeks to months.
Address biomechanics first; even pressure-positive anterior CECS may improve sufficiently with structured gait retraining to avoid surgery.
Return to sport/work: After fasciotomy, return-to-sport ranges widely (~26–100%) with satisfaction ~42–94%; open vs endoscopic shows similar outcomes overall. 12,16,17
Conservative success: Gait retraining programs in military/runner cohorts show meaningful symptom resolution and reduced surgery rates in many patients. 5
Poor prognostic indicators: Deep posterior involvement, multiple compartments, military occupation, and need for revision fasciotomy have been associated with lower satisfaction/RTS in some series. 12,15,17
References
Vogels S, Ritchie ED, van der Burg BLSB, et al. Clinical Consensus on Diagnosis and Treatment of Patients with Chronic Exertional Compartment Syndrome of the Leg: A Delphi Analysis. Sports Med. 2022;52(12):3055-3068. (SpringerLink)
Roscoe D, Roberts AJ, Hulse D. Intramuscular Compartment Pressure Measurement in Chronic Exertional Compartment Syndrome: New and Improved Diagnostic Criteria. Am J Sports Med. 2015;43(2):392-398. (upload.orthobullets.com)
Maksymiak R, Ritchie E, Zimmermann W, et al. Historic cohort: outcome of CECS-suspected patients. BMJ Mil Health. 2021;167(6):387-393. (militaryhealth.bmj.com)
Freedman BA, et al. Return to Sport After Fasciotomy for Forearm CECS: Systematic Review. Am J Sports Med. 2024. (CoLab)
Zimmermann WO, Hutchinson MR, van den Berg R, et al. Conservative treatment of anterior CECS in the military with mid-term follow-up. BMJ Open Sport Exerc Med. 2019;5:e000532. (BMJ Open Sports & Exercise Medicine)
Hartman J, Simpson S. Current Diagnosis and Management of CECS. Curr Phys Med Rehabil Rep. 2018;6:136-141. (SpringerLink)
Ringler MD, et al. MRI accurately detects CECS: validation study. Skeletal Radiol. 2012;42:385-392 (supporting modality use in modern reviews). (SpringerLink)
Baria MR, Sellon JL. Botulinum toxin for CECS: case report with 14-month follow-up. Clin J Sport Med. 2016. (SpringerLink)
MIRROR project summary; case series data on BoNT-A for CECS. 2022. (mirrorusuhs.org)
Hurley ET, et al. Return to sport & outcomes after open vs endoscopic release for CECS. Arthrosc Sports Med Rehabil. 2022;4(6):e1913-e1920. (ScienceDirect)
Beldame J, Prado G. Endoscopic fasciotomy for forearm CECS—outcomes. World J Orthop. 2021;12(5):320-331. (WJGNET)
Hsu RY, et al. Rehabilitation and return-to-activity criteria after CECS surgery: systematic review. Physician Sportsmed. 2023;52(2):125-133. (Europe PMC)
Campano D, et al. Systematic review of fasciotomy in CECS (complications & revisions). J Vasc Surg. 2020;71:1541-1552. (jvascsurg.org)
Waterman BR, et al. Risk factors & outcomes in military populations. Clin Sports Med. 2014;33:693-705; plus related analyses. (Context for prognosis/recurrence in military). (sportsmed.theclinics.com)










Discussion