Inguinal Hernia

Higher incidence among men 40 to 59 years of age. Although there are many different types of hernias, they are usually related to the abdomen, with approximately 75% of all hernias occurring in the inguinal region. Hernia contains omentum (90% of cases) or intestine (10% of cases). Inguinal hernias are at risk of irreducibility or incarceration, which may result in strangulation and obstruction. However, femoral hernias are much more likely to strangulate compared to inguinal because of the narrowed femoral ring.
Hernia: A bulge or protrusion of an organ or tissue through an abnormal opening within the anatomic structure that normally confines it.
Inguinal Hernia:
Reducible: Refers to a hernia that can be moved back into place easily (either manually or spontaneously)
Irreducible: Refers to a hernia that CANNOT be moved back into place, remains budged. Irreducible hernia can lead to a incarcerated, obstructed or strangulated hernia.Incarcerated: Refers to a hernia that cannot be pushed back. It does not necessarily mean that the hernia is strangulated or that obstruction is occurring (although both are possible). If spontaneously reduced, and patient feels better.
Obstructed hernia: gut hernia causing incarceration (momentum hernia does not cause incarceration because gut flow is normal)
Strangulated hernia: compression of blood flow to the strangulated bowel leading to necrosis
The composition of a hernia is 1. the sac, 2. the covering of the sac 3. the content of the sac.
| “No disease of the human body, belonging to the province of the surgeon, requires in its treatment a better combination of accurate anatomical knowledge with surgical skill than Hernia in all its varieties” Astley Cooper (1804) |
Inguinal Hernia Anatomy
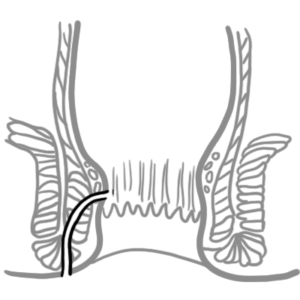
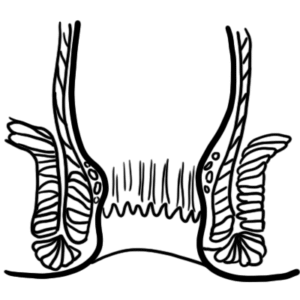
The inguinal canal is the oblique passage through the lower abdominal wall. It runs from deep to superficial, from internal to external inguinal rings. The testis follows this canal and into the scrotum during development, and therefore the spermatic cord runs through this canal.
The deep and superficial ring should close normally
Mid-inguinal point (between the ASIS and pubic symphysis): Femoral artery
Mid point of the inguinal point (between the ASIS and pubic tubercle): deep ring of the inguinal canal
Borders of the Inguinal Canal
Contents of the Inguinal Canal (rule of 3s)
in females the content of the inguinal canal is four things: Round ligament, genital branch of the genitofemoral nerve, lymphatics and sympathetic plexus.
Borders of the Hesselbach Triangle
| Indirect Inguinal | Direct Inguinal | Femoral | |
| Definition | Intestine passes through deep inguinal ring | Intestine passes through weak abdominal wall | Intestine passes through weak femoral ring |
| Age | Any age but usually young | Acquired weakness in abdominal wall | More common in women, due to their wider bony pelvis |
| Aetiology | Congenital (patent process vaginalis) | Acquired | Acquired |
| Relationship to inferior epigastric artery | Lateral | Medial | An aberrant obturator artery of the inferior epigastric arery ,ay cross the lacunar ligament |
| Descending to scrotum | Often | Rarely | – |
| Occluding the internal ring | Controls it | Does not control it | – |
| Neck | Narrow | Wide | Narrow |
| Strangulation | More likely | Rare | Much more likely |
| Treatment | Infant – herniotomy, Adults – open/laparoscopic mesh | Open/laparoscopic mesh | Laparoscopic mesh |
Aetiology
Hernia occur at sites of weakness in the wall. This weakness may be:
In terms of inguinal herniae:
The diagnosis of an inguinal hernia is usually made through history and physical examination findings. Patients can either be asymptomatic or symptomatic
Asymptomatic with a bulge
Symptomatic with a buldge- Gradually or suddenly
Examination
Hernias may be easily diagnosed with an adequate physical examination.
Bilateral inguinal hernias are extremely common, as is clinically evident connective tissue weakness in both groins. Any patient presenting with an inguinal hernia should have the contralateral groin examined when lying flat.
Red Flag Triad: Irreducible, Absent cough impulse, Pain
Differential Diagnosis
| DIFFERENTIAL DIAGNOSIS OF SCROTAL/GROIN LUMP | |
| Condition | Clinical features |
| Ectopic testis | Absence of a testis in the scrotum |
| Epididymitis | Severe pain surrounding the testis, tenderness, fever, chills |
| Femoral adenitis/adenopathy | Bilateral, firm, tender nodes; fever |
| Femoral arterial aneurysm | Older patient, pulsatile mass, no systemic symptoms |
| Femoral hernia | More common in women, often incarcerated, bowel obstruction |
| Hematoma | Associated trauma, ecchymoses, tenderness, no change with Valsalva maneuver |
| Hidradenitis | Draining abscesses in intertriginous skin of the groin |
| Hydrocele | Mass in the scrotum or inguinal canal that transilluminates |
| Inguinal adenitis/adenopathy | Tenderness, redness possible, often bilateral, systemic symptoms |
| Inguinal hernia | Bulge or impulse detected in inguinal canal with Valsalva maneuver or coughing |
| Lymphoma | Firm, tender mass; may increase in size; organomegaly; systemic symptoms |
| Lipoma | Soft, asymptomatic mass; does not change in size |
Non-Surgical Treatment
Surgical Treatment (recommended)
| LAPROSCOPIC SURGERY | |
| Advantages | Disadvantages |
| Quicker recovery time than open repair — usually about half the time to activity. | Rarely, unrecognised bowel perforation caused by balloon inflation has occurred when dense adhesions after peritonitis have tethered the bowel |
| Less postoperative pain has been shown in several series | More expensive than open repair |
| Less chronic groin pain — the surgery takes place behind the muscles, so no nerves are likely to be damaged | Future prostate cancer surgery is very difficult for the urologist, as the pre-peritoneal space anterior to the bladder is obliterated |
| Less risk of damage to the testicular blood supply | A general anaesthetic is always required |
Complication of hernia
Complication of Surgery
Jenkins, JT 2008, Inguinal hernias, BMJ, vol. 336, no. 7638, pp. 269-272.
Phillips, DJ 2006, How to Treat, Australian Doctor.










Discussion