Overview
Sarcoidosis is a multisystem granulomatous disease of unknown cause, characterised by the formation of non‑caseating granulomas in affected organs. Pulmonary involvement occurs in ~90% of patients, making it the most common manifestation. Global prevalence varies widely (e.g., 3.7/100,000 in Japan vs. 28.2/100,000 in Finland), with higher rates in Black Americans and Northern Europeans. Peak onset is between 20–40 years, with a female predominance. Risk factors include genetic susceptibility (HLA‑DRB1 alleles), environmental exposures (inhaled antigens, bioaerosols), and certain occupations (firefighting, metalworking). Major complications of pulmonary sarcoidosis include pulmonary fibrosis, pulmonary hypertension, and respiratory failure.
Definition
Sarcoidosis: Multisystem inflammatory disease with non‑caseating granulomas.
Non‑caseating granuloma: Organised collection of epithelioid histiocytes without central necrosis.
Pulmonary fibrosis: Irreversible scarring of lung parenchyma.
Pulmonary hypertension: Elevated pulmonary artery pressure, often secondary to chronic lung disease.
Anatomy and Physiology
- Respiratory tract divisions: Upper airways, conducting bronchi, terminal bronchioles, respiratory bronchioles, alveoli.
- Alveolar–capillary interface: Site of gas exchange; thin barrier for O₂/CO₂ diffusion.
- Lymphatic drainage: Peribronchovascular and subpleural lymphatics drain to hilar and mediastinal nodes.
- Immune surveillance: Alveolar macrophages and dendritic cells present antigens to T‑cells in lymph nodes.
Aetiology and Risk Factors
Aetiology
- Unknown; likely multifactorial.
- Proposed triggers: microbial antigens (mycobacteria, propionibacteria), inorganic dusts, bioaerosols.
- Aberrant immune response in genetically predisposed individuals.
Risk Factors
- Genetic: HLA‑DRB1*03, *14, *15.
- Ethnicity: Black Americans, Northern Europeans.
- Age: 20–40 years.
- Female sex.
- Occupational: firefighting, metalworking, agricultural dust exposure.
- Family history of sarcoidosis.
Pathophysiology
- Trigger exposure in susceptible host.
- Antigen presentation by alveolar macrophages/dendritic cells to CD4+ T‑cells.
- Th1‑mediated immune response → release of IL‑2, IFN‑γ.
- Macrophage activation → TNF‑α production.
- Granuloma formation in lung parenchyma and lymph nodes.
- Resolution in many cases; in others, chronic inflammation → fibrosis and architectural distortion.
Clinical Manifestations
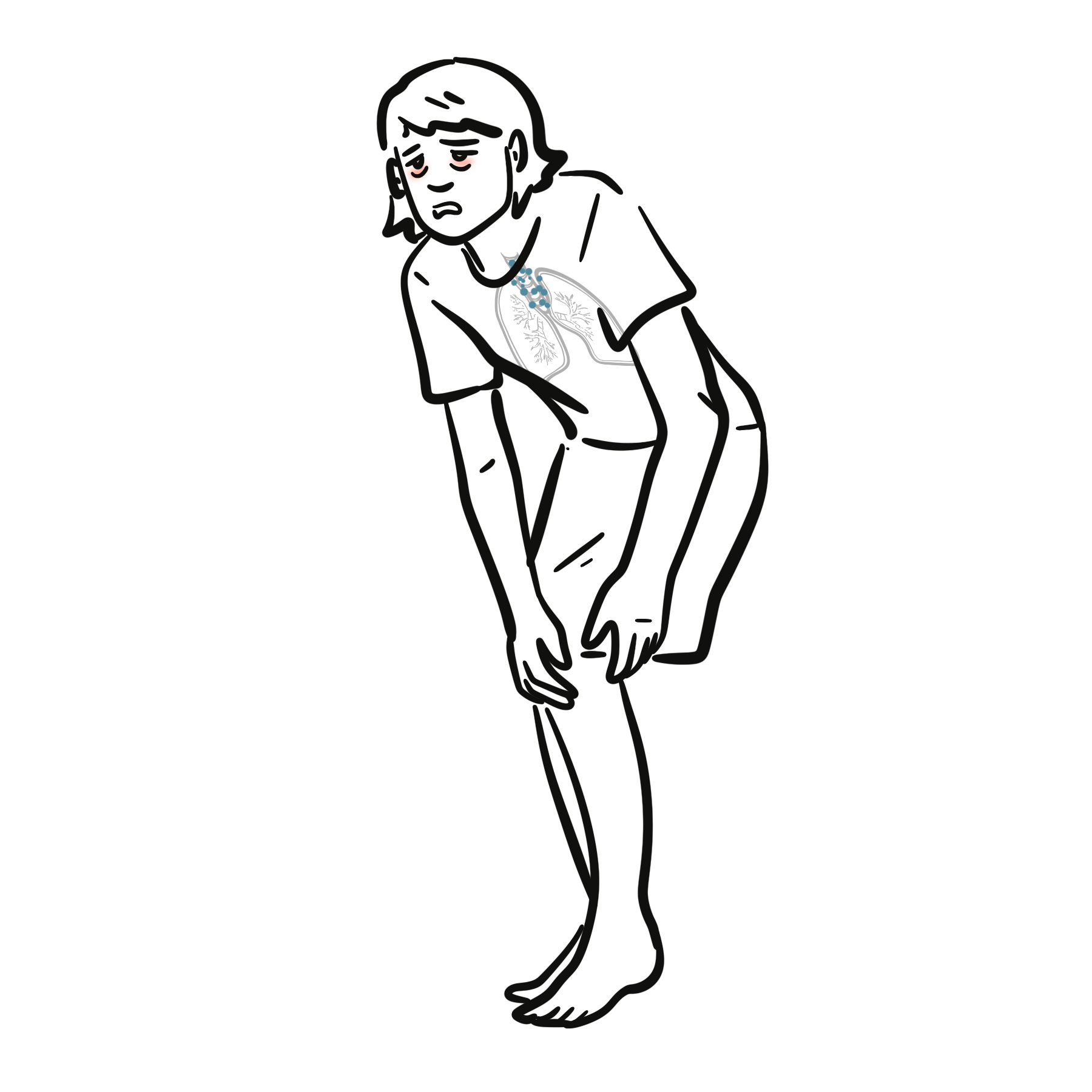
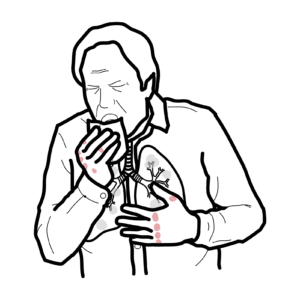
- Respiratory: Dry cough, progressive dyspnoea, chest discomfort.
- Systemic: Fatigue, weight loss, fever.
- Examination: Often normal; may have crackles (fibrosis), clubbing (late), signs of pulmonary hypertension.
- Radiographic hallmark: Bilateral hilar lymphadenopathy ± parenchymal infiltrates.
Respiratory exam can be normal despite significant radiographic disease.
Diagnosis
Diagnostic approach: Compatible clinical/radiological picture + histological evidence of non‑caseating granulomas + exclusion of other causes.
Investigations
- CXR: Staging (I–IV).
- HRCT: Parenchymal nodules, fibrosis, lymphadenopathy.
- PFTs: Restrictive defect, ↓DLCO.
- Serum ACE (non‑specific), hypercalcaemia.
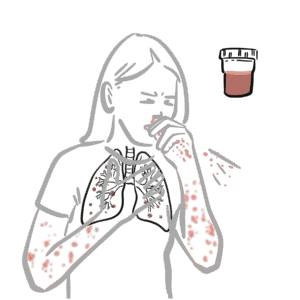
- Bronchoscopy with transbronchial biopsy or EBUS‑TBNA.
Differential Diagnosis
- Tuberculosis
- Lymphoma
- Hypersensitivity pneumonitis
- Berylliosis.
Classification
By radiographic stage (Scadding):
- Stage I: Bilateral hilar lymphadenopathy (BHL) only.
- Stage II: BHL + parenchymal infiltrates.
- Stage III: Parenchymal infiltrates without BHL.
- Stage IV: Pulmonary fibrosis.
Treatment
- Observation: Many cases resolve spontaneously (esp. Stage I).
- Indications for treatment: Symptomatic, progressive lung disease, extrapulmonary organ threat.
- First‑line: Oral corticosteroids taper (prednisolone).
- Steroid‑sparing agents: Methotrexate (first-line), azathioprine, mycophenolate.
- Refractory disease: Anti‑TNF agents (infliximab).
- Supportive: Pulmonary rehab, oxygen, manage comorbidities.
Avoid overtreatment; weigh steroid risks vs. benefits.
Complications and Prognosis
Complications
- Pulmonary fibrosis.
- Pulmonary hypertension.
- Chronic respiratory failure.
- Increased infection risk (immunosuppression).
- Bronchiectasis.
Prognosis
- ~2/3 achieve remission within 10 years.
- Poor prognostic factors: Stage IV disease, Black ethnicity, chronic progressive course, pulmonary hypertension.
References
- Thillai M, et al. BTS Clinical Statement on pulmonary sarcoidosis. Thorax. 2020;76(1):4‑20.
- Baughman RP, et al. Diagnosis and Treatment of Pulmonary Sarcoidosis: A Review. JAMA. 2021;326(9):890‑900.
- Judson MA. The Clinical Features of Sarcoidosis: A Comprehensive Review. Clin Rev Allergy Immunol. 2015;49(1):63‑78.
- Spagnolo P, et al. Pulmonary sarcoidosis. Lancet Respir Med. 2018;6(5):389‑402.
















Discussion