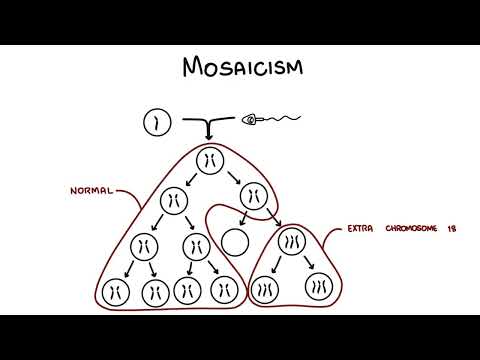
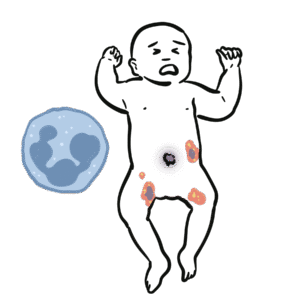
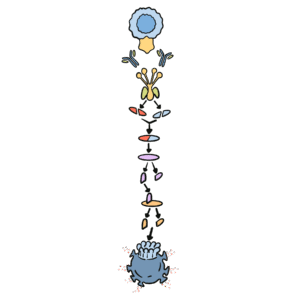
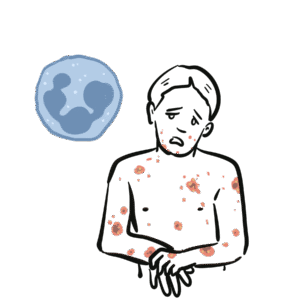
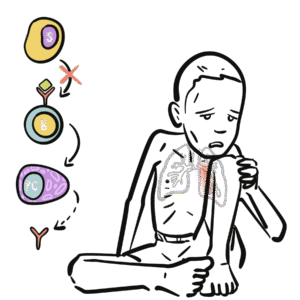
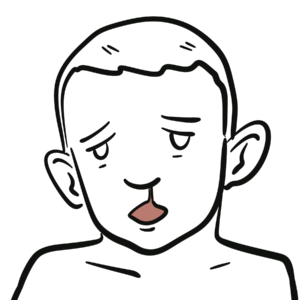
0:00 Angelman's syndrome is a rare genetic condition which affects approximately 1 0:08 in 12 to 20,000 0:10 people, although many cases go undiagnosed. 0:14 Angelman's syndrome is caused by deficient gene expression of E3 ubiquitin 0:18 protein ligase, 0:19 also known as UBE3A, and was first described in 1965 by Dr. Harry Angelman. 0:28 Electric findings of Angelman's syndrome include severe developmental delay and 0:31 movement or 0:32 balanced disorder, usually in the form of gaitataxia and/or tremulous movement 0:38 of limbs. 0:39 Now let's talk about some genetics to better understand Angelman's syndrome. 0:47 Typically a person has 46 chromosomes that make up each cell, 23 from mom and 0:52 23 from 0:53 dad, the 23 from mom and 23 from dad are paired, for a total of 46 chromosomes 1:01 in each cell. 1:03 As an example here, you have two pairs of chromosome 15. 1:09 Now the sex cells which are the male sperm and female egg are produced through 1:12 a process 1:13 called meiosis. 1:14 Let us follow the maternal sex cells, so looking at the mom's egg and how they 1:21 are produced. 1:23 The 46 chromosomes will first duplicate or replicate initially. 1:29 Through meiosis, they then divide to form two cells with 23 chromosomes. 1:40 The 23 chromosomes are still duplicated, then meiosis two occurs where the 1:47 chromosomes 1:48 separate and then you form the sex cells, each with 23 chromosomes but single 1:55 chromosomes 1:57 and they are no longer duplicated. 2:00 The male sex cell, the sperm, will have 23 chromosomes which then fertilizes 2:07 the egg 2:07 and the baby is born with 46 chromosomes, 23 from mom and 23 from dad. 2:15 Angelman syndrome is caused by deficient gene expression of E3 ubiquitin 2:20 protein ligase, 2:21 also known as UBE3A. 2:24 This gene is located on chromosome 15. 2:27 Normally, the UBE3A gene, inherited maternally, is active and the copy of the 2:34 gene, inherited 2:36 from the father, is silenced. 2:39 This is a phenomenon known as imprinting. 2:42 In Angelman syndrome, the maternal copy of the gene is malfunctioning, 2:46 resulting in deficient 2:47 gene expression of E3 ubiquitin protein ligase. 2:53 The E3 ubiquitin protein ligase is a critical enzyme involved in proteasome 2:58 mediated protein 2:59 degradation, which is essentially a important function for cells to degrade 3:08 proteins. 3:10 Now most cases of Angelman syndrome are caused by deletion, meaning they are 3:15 missing a part 3:16 of the DNA in the region of chromosome 15, on the maternal chromosome 15. 3:22 Other causes include a mutation in this area, uni, parental disome, where you 3:29 have two copies 3:30 of chromosome 15 from the father, so nothing from the mom, and imprinting 3:36 defect, which 3:37 occurs when the maternal chromosome 15 is blank. 3:42 Most cases of Angelman syndrome are not inherited, especially those caused by 3:46 mutations or uni 3:48 parental disome. 3:50 Instead they are caused by random events during the formation of the sex cells 3:56 or in early 3:57 embryonic development. 4:00 Angelman syndrome affects both males and females equally. 4:04 And so as a result of the mutation or deletion in chromosome 15, you get 4:11 deficient gene expression 4:14 of the UBE3A gene, an important enzyme involved in proteasome mediated protein 4:21 degradation. 4:22 And because of that, you get Angelman syndrome and the clinical features of 4:28 Angelman syndrome. 4:29 Now Angelman syndrome is a neurodevelopmental disorder. 4:32 There is a broad spectrum of symptoms associated with Angelman syndrome, and it 4:36 is often misdiagnosed 4:38 as cerebral palsy or autism. 4:40 Typical characteristics are usually not evident at birth. 4:44 Children with the syndrome may have feeding difficulties as infants and 4:47 developmental 4:48 delay is often noticeable around 6-12 months of age. 4:53 Milestones in motor development such as walking are often delayed. 4:56 A common early finding is ataxia, which is difficulty with balance, jerking and 5:02 tremulous 5:02 movements of the limbs. 5:05 Children often have hand flapping movements. 5:09 Communication difficulties are common, and most children are not able to speak 5:12 more than 5:12 a few words. 5:14 Children also have a behavioral pattern, which includes a happy and excitable 5:19 demeanor, often 5:20 laughing and smiling. 5:22 Micro and carefully and seizures are also common. 5:25 Some other features include facial features, which include a prominent chin, 5:29 deep set eyes, 5:30 abnormally white mouth, called macrostomia, with a protruding tongue, widely 5:36 spaced teeth, 5:37 and an abnormally flat part of the skull, breaking carefully. 5:41 Adults may have minimal pro-genthism, a prominent lower jaw. 5:45 People with Angelman syndrome have a fascination with water, a love for music 5:50 and attraction 5:50 to shiny objects. 5:52 It can also be sensitive to heat, and most have disruptive sleep cycles. 6:02 There are associated complications of Angelman syndrome, and this includes 6:06 constipation 6:07 or gastro-sophageal reflux disorder, strabismus, hypopigmentation causing phot 6:13 ophobia, nystagmus 6:15 and decreased visual acuity, sleep disturbances as I've mentioned, progressive 6:20 scoliosis, 6:21 and contractures and obesity later in life. 6:30 Diagnosis and Investigation 6:32 As the characteristic findings of Angelman syndrome are often not apparent at 6:36 birth, diagnosis 6:37 is usually made between 1 and 4 years of age. 6:41 Majority of cases can be confirmed through highly specialized blood tests, such 6:45 as DNA 6:45 methylation and fluorescent in situ hybridization, also known as fish, or micro 6:52 array chromosome 6:52 analysis, is able to detect the characteristic deletion of chromosome 15, that 6:58 is seen in 6:59 majority of Angelman syndrome cases. 7:03 Mutation analysis of UBE3A can be helpful for diagnosis in patients who have 7:08 negative DNA 7:09 methylation studies. 7:12 The counseling is recommended for all families affected by Angelman syndrome. 7:21 Treatment of Angelman syndrome then focuses on symptomatic management and 7:25 supportive care, 7:26 and involves a multi-disciplinary team. 7:29 There's currently no genetic therapy or curative medication available. 7:33 Early intervention is essential, and most children benefit greatly from 7:36 physical, speech, 7:37 and occupational therapy, as well as behavioral modification therapy. 7:42 Some specific treatment and management include anti-seizure medications, 7:46 behavioral therapy 7:47 and bedtime routines to manage the associated sleep disorders, modified 7:53 breastfeeding methods 7:54 and devices which can help infants with breastfeeding difficulties, gastroesoph 7:59 ageal reflux management 8:00 can be with positioning or with medication, laxatives of constipation, ankle 8:06 braces and 8:07 mobility devices, including physiotherapy to help with scoliosis, use of 8:13 special communication 8:15 devices to help communicate and learn, surgical correction of strabismus. 8:27 Last span for people with Angelman syndrome is usually normal compared to that 8:30 of the 8:30 general population, and young adults generally have good physical health. 8:36 However, some issues such as seizures and abnormal movements may continue into 8:41 adulthood, 8:42 and living independently is not possible for adults who have these symptoms. 8:53 So in summary, today we talked about Angelman syndrome, a genetic disorder that 8:56 is caused 8:57 by deficient gene expression of E3 ubiquitin protein ligase, also known as UBE3 9:03 A on chromosome 9:04 15. 9:05 We discussed the genetics, clinical features of the syndrome, as well as the 9:09 process of 9:10 diagnosis, management and prognosis. 9:14 Thank you for watching. 9:27 You