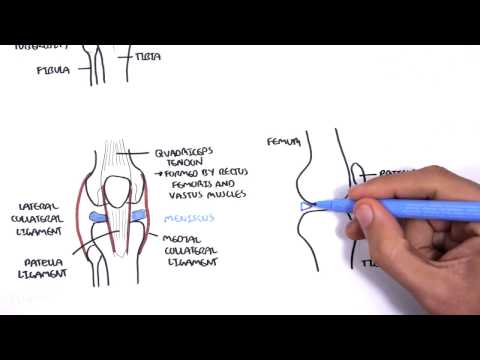
0:00 The femur is the longest and heaviest bone in the body. 0:12 It transmits body weight from the hip bone to the tibia when the person is 0:16 standing. 0:17 Its length is approximately a quarter of the person's height. 0:20 The femur consists of the shaft, which is the body, and the two ends, the prox 0:25 imal and 0:26 distal ends of the femur. 0:33 Let's first talk about the proximal end of the femur, or also known as the 0:38 superior end. 0:41 The proximal end of the femur consists of the head, neck, and two trochanters, 0:46 the graded 0:46 trochanter and the lesser trochanter. 0:50 The head of the femur is round, and it articulates with the acetabulum of the 0:57 pelvis to form 0:58 the hip joint. 1:01 The femoral head is covered with articular cartilage, except for immediately 1:06 placed depression 1:08 or pit the fovea for the ligament of the head. 1:11 In early life, the ligament gives passage to an artery, supplying the epiphysis 1:21 of the head. 1:22 The neck of the femur connects the head of the femur with the shaft. 1:27 The neck of the femur is a common sight for fractures. 1:31 The intratrokenteric line is a sight where the neck and the shaft join. 1:36 It is a roughened ridge formed by the attachment of a powerful ligament, the 1:41 ileophimoral ligament. 1:47 Now focusing on the shaft of the femur. 1:50 The shaft of the femur descends in a slight medial direction, and this brings 1:55 the knees 1:55 closer to the body's center of gravity, increasing stability. 2:05 In clinical anatomy, fractures of the femur. 2:11 Despite its large size and strength, the femur is commonly fractured, and the 2:14 most common 2:15 fractures include the neck of the femur, intratrokenteric fractures, and shaft 2:20 fractures. 2:21 The neck of the femur is the most common sight for fractures, because it is the 2:24 narrowest 2:25 and weakest part of the bone. 2:27 The most common cause of fractures is trauma, usually, and a major risk factor 2:32 is osteoporosis, 2:33 which is the weakening of the bones, and this makes it more prone to fractures. 2:43 Now talking about the distal end of the femur. 2:48 Here you find what's called the medial and lateral condiles. 2:53 The femoral condiles articulate with the meniscae, which is cartilage, and the 2:59 tibial condiles 3:00 themselves to form what's called the knee joint. 3:04 The medial and lateral epicondiles, epi as in above, the epicondiles provide 3:09 proximal 3:10 attachment for the medial and lateral collateral ligaments of the knee joint. 3:19 Then you have the intercondylophosa, and the patellar surface. 3:25 Now the condiles themselves are separated posteriorly and inferiorly by an 3:32 intercondylophosa. 3:34 But merge anteriorly when you look at the front, it merges, forming a 3:39 depression called 3:41 the patellar surface. 3:44 And this surface is what articulates with the patellar bone. 3:49 The intercondylophosa contains two facets for the attachment of the intracaps 3:54 ular knee 3:55 ligaments, the anterior cruciate ligament ACL, and the posterior cruciate lig 4:00 ament PCL. 4:08 Now going back to the proximal end of the femur, the proximal femur is bent in 4:15 an L-shaped, 4:17 so that the long axis of the head and neck projects superior medially at an 4:23 angle to 4:24 that of an obliquely oriented shaft. 4:32 This obtuse angle of inclination is greatest, most nearly straight at birth, 4:38 and then it 4:39 gradually diminishes, becomes more acute until adulthood, and the angle that is 4:46 reached on 4:47 average is about 126 degrees. 4:55 The angle of inclination also increases with age, and this also contributes to 5:01 the increased 5:02 risk of fracture. 5:03 However, in females, the angle of inclination is less, and this is because of 5:07 the increase 5:08 width between the acetabula and the greater oblique orientation of the femoral 5:15 shaft. 5:16 The angle of inclination allows greater mobility of the femur at the hip joint. 5:28 Some clinical anatomy, cocsavara and cocsavalga. 5:32 Now the angle of inclination between the long axis of the femoral neck and the 5:37 femoral 5:38 shaft, it varies with age, sex and development of the femur. 5:44 When the angle of inclination is decreased, the condition is cocsavara. 5:50 When it is increased, it is known as cocsavalga. 5:54 Varra is a Latin term which describes any bone or joint that is deformed in 5:59 such a way 5:59 that its distal element is deviated towards midline, so in cocsavara there is 6:06 increased 6:07 joint stability due to increased coverage of the femoral head in the acetabulum 6:12 . 6:13 People will tend to have knocked knees, so the knees are brought together. 6:18 The term valga is used when the distal element deviates away from the midline, 6:24 so people 6:25 will have what's called bow legs, so the knees are quite separated. 6:35 The angle of declination. 6:38 Now when the femur is viewed from the top, so superiorly, you're looking down 6:43 at the 6:44 shaft and the head here, it is apparent that the two axis lies at an angle, and 6:50 this is 6:51 the torsion angle or angle of declination. 6:57 The average in males is about 7 degrees and in females is 12 degrees. 7:02 When you have anti-version, excessive anti-version, this is an increase in the 7:07 angle of the femoral 7:09 torsion, while a decrease in the angle of femoral torsion is known as retro 7:15 version. 7:16 Now these changes the biomechanics of walking and standing as depicted by the 7:20 foot stance 7:21 in this image. 7:25 So you can see in these images with excessive anti-version the foot will be 7:30 medial stance 7:31 and in retroversion the foot will be in an external stance. 7:35 Now let's briefly talk about the blood supply of the femur. 7:42 The femoral artery, which is a continuation of the external iliac artery, 7:47 constitutes the 7:48 major blood supply to the lower limb. 7:51 The femoral artery gives off profound ephemeris, a branch below the inguinal 7:56 ligament and becomes 7:58 also the other the superficial femoral artery. 8:02 The superficial femoral artery ends as it passes through the adductor hiatus in 8:07 adductor 8:08 magnets to continue as a public teal artery. 8:17 Blood supply of the neck and head of femur is a bit more complicated. 8:23 The majority of blood supply to the head and neck of the femur comes from the 8:26 medial and 8:27 lateral circumflex branches of the profundar femoris, so the deep femoral 8:33 artery. 8:35 The medial and lateral circumflex femoral arteries are nastomose to form a ring 8:39 around 8:40 the neck of the femur. 8:43 And from here you have small arteries branching off to perfuse the femoral head 8:49 . 8:49 Now this is the main blood supply for the femoral head. 8:54 Another direct source of supply to the femoral head is from the folvial artery, 8:59 which only 9:00 occurs in the pediatric population, because eventually this is replaced by the 9:06 ligamentum 9:07 terrace, as we have learned earlier. 9:09 The ligamentum terrace is the ligament connecting the head of the femur to the 9:15 acetabulum. 9:16 Now there are two important anastomoses that provide collateral blood flow to 9:22 support the 9:22 femoral head. 9:24 One is the cruciate anastomosis, which is between the inferior gluteal artery 9:28 and the 9:29 medial circumflex femoral artery. 9:31 And the other is the trochanteric anastomosis, which is between the superior gl 9:36 uteal artery 9:37 and the medial and lateral circumflex femoral arteries. 9:46 Some clinical anatomy, avascular necrosis of the femoral head. 9:50 Avascular necrosis or osteonacrosis of the femoral head is characterized by 9:55 bone cell 9:55 death that follows an impairment of blood flow to the bone. 9:59 And this could be due to a traumatic or non-traumatic cause. 10:04 As we have learned, the blood vessels supplying the femoral head rely on small 10:09 arteries with 10:10 limited collateral blood flow. 10:17 So in summary, in this video we discussed the anatomy of the femur and its 10:21 blood supply. 10:22 The femur is divided into the proximal, shaft and distal segments. 10:26 The proximal femur is a common site for femoral fractures. 10:30 The angle of inclination is an obtuse angle between the long axis of the fem 10:34 oral neck and 10:36 femoral shaft, averaging an adult of 126 degrees. 10:40 Largely in the angle can lead to coxavara and/or coxavalca.