

Fibromyalgia
Overview
Fibromyalgia is a chronic, nociplastic pain condition characterised by widespread pain with prominent fatigue, sleep disturbance, and cognitive symptoms, reflecting altered central pain processing rather than tissue injury. Global prevalence is ~2–4%, higher in women, ages 20–60, and in those with mood/sleep disorders, obesity, low socioeconomic status, and comorbid rheumatic disease. Major complications include functional impairment, work disability, polypharmacy, and elevated risks of depression and suicidality; timely, multimodal, non-pharmacological care improves outcomes 2,5,15.
Definition
Nociplastic pain: pain from altered nociception without clear evidence of ongoing tissue damage or somatosensory lesion
Central sensitisation: increased responsiveness of nociceptive neurons in CNS to normal/subthreshold input, manifesting as hyperalgesia/allodynia
WPI (Widespread Pain Index): count (0–19) of painful body sites over past week used in ACR criteria
SSS (Symptom Severity Scale): 0–12 score (fatigue, waking unrefreshed, cognitive symptoms + somatic symptoms) used in ACR criteria
Classification
Chronic pain is now categorised according to the International Classification of Diseases, 11th Revision (ICD-11) into two main groups: chronic primary pain and chronic secondary pain. This classification helps distinguish pain as a disease in itself versus pain as a symptom of another condition.
Chronic Primary Pain
- Definition: Pain that persists for ≥3 months and is not better explained by another condition. It is considered a disease in its own right, often associated with emotional distress or functional disability.
- Examples
- Chronic widespread pain (CWP)
- Fibromyalgia
- Complex regional pain syndrome (CRPS)
- Chronic primary headache
- Chronic primary visceral pain (e.g., irritable bowel syndrome)
- Chronic primary musculoskeletal pain (e.g., non-specific low back pain)
Chronic Secondary Pain
- Definition: Pain that arises as a symptom secondary to an underlying disease.
- Subtypes:
- Chronic cancer-related pain
- Chronic postsurgical or post-traumatic pain
- Chronic neuropathic pain (e.g., diabetic neuropathy)
- Chronic secondary musculoskeletal pain (e.g., due to osteoarthritis or rheumatoid arthritis)
- Chronic secondary visceral pain (e.g., due to endometriosis)
- Chronic secondary headache or orofacial pain
Anatomy & Physiology
- Ascending nociceptive pathways: peripheral A-delta/C fibres → dorsal horn → spinothalamic/limbic projections → thalamus → primary/secondary somatosensory cortices, insula, ACC.
- Descending modulation: periaqueductal grey–rostral ventromedial medulla pathways inhibit/facilitate dorsal horn transmission via serotonin, noradrenaline, endogenous opioids.
- Sleep–pain interface: slow-wave sleep maintains descending inhibition; sleep loss augments temporal summation.
- Autonomic–HPA axis: sympathetic arousal and cortisol rhythms modulate pain thresholds and fatigue.
Pain intensity ≠ tissue damage; disability is driven by sensitisation, sleep and mood dysregulation.
Ask about sleep quality and exercise tolerance—changing these often shifts pain more than escalating analgesics.
Aetiology & Risk Factors
Aetiology (multifactorial, biopsychosocial)
- CNS hyperexcitability and impaired descending inhibition (nociplastic pain)
- Neuroinflammation/glial activation in pain networks (PET evidence)
- Small-fibre pathology in a subset (reduced intra-epidermal nerve fibre density)
- Dysregulated stress systems: autonomic (sympathetic overactivity) and HPA axis alterations
- Genetic/familial susceptibility with environmental triggers (infection, trauma, major stress)
- Female sex, middle age
- Insomnia/sleep apnoea
- Depression/anxiety
- Obesity/inactivity
- Adverse childhood experiences (PTSD)
- Catastrophizing
- Low socioeconomic status
- Comorbid rheumatic or pain disorders
- Viral illness or physical trauma as precipitant
Coexisting inflammatory disease (e.g., RA, SLE) is common—active inflammation and fibromyalgia can co-occur and amplify patient-reported disease activity.
Pathophysiology
- Predisposition (genes, sex hormones, early adversity) → heightened pain gain setting.
- Trigger (infection, trauma, psychosocial stress, poor sleep) → increased peripheral input + stress reactivity.
- CNS changes: augmented temporal summation, impaired conditioned pain modulation, altered connectivity/chemistry in insula–ACC–DMN; glial activation and pro-inflammatory signalling sustain hyperexcitability
- Systemic correlates: autonomic dysregulation (orthostatic symptoms), HPA rhythm changes, microglial cytokines, altered neurotransmitters (↓NA/5-HT; ↑glutamate)
- Clinical expression: widespread pain, sensory hypersensitivity, fatigue, sleep/cognitive symptoms; in a subset, small-fibre pathology contributes to dysaesthesias 9.
“Low phosphate” or raised CRP/ESR is not expected—abnormalities suggest an alternative or additional diagnosis.
Clinical Manifestations
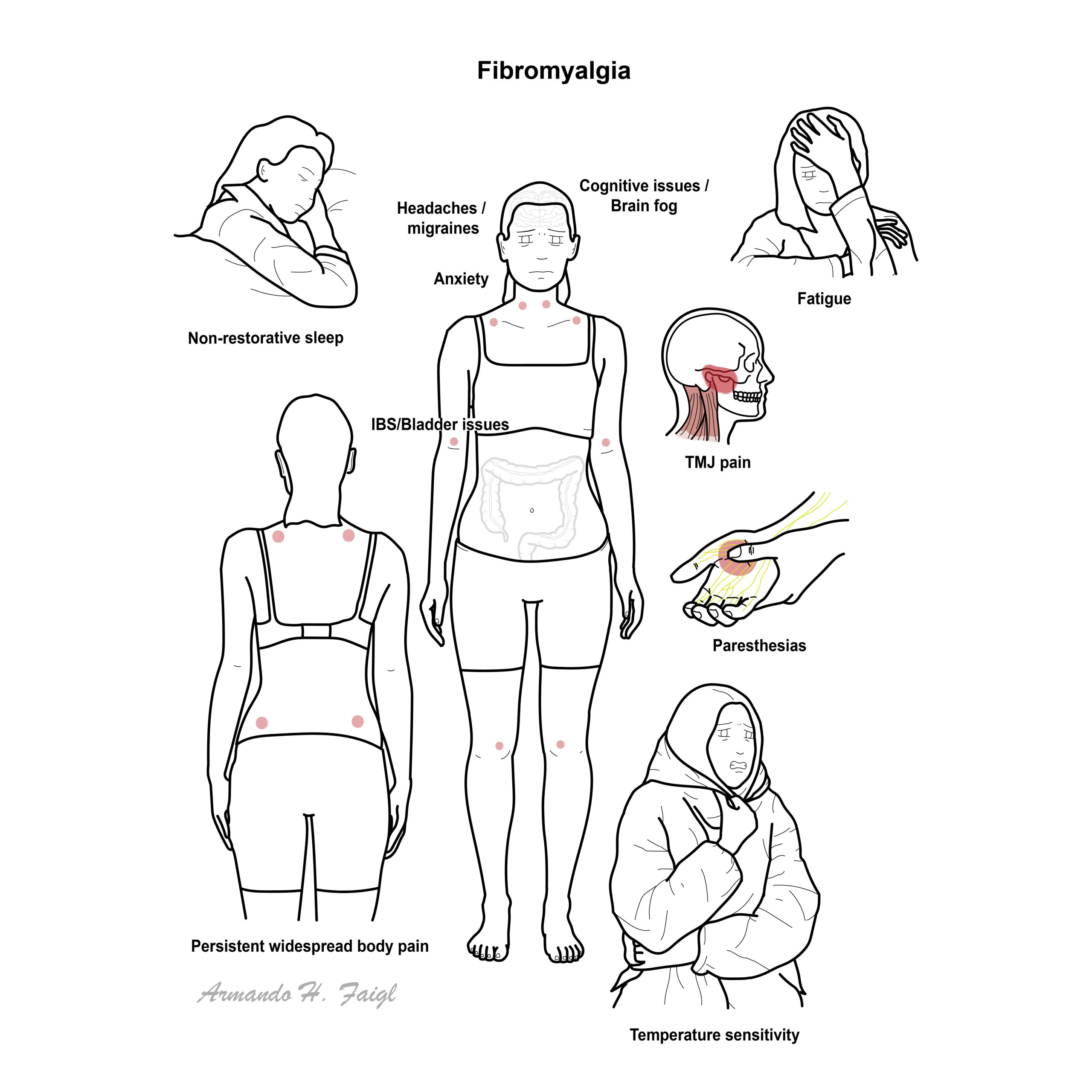
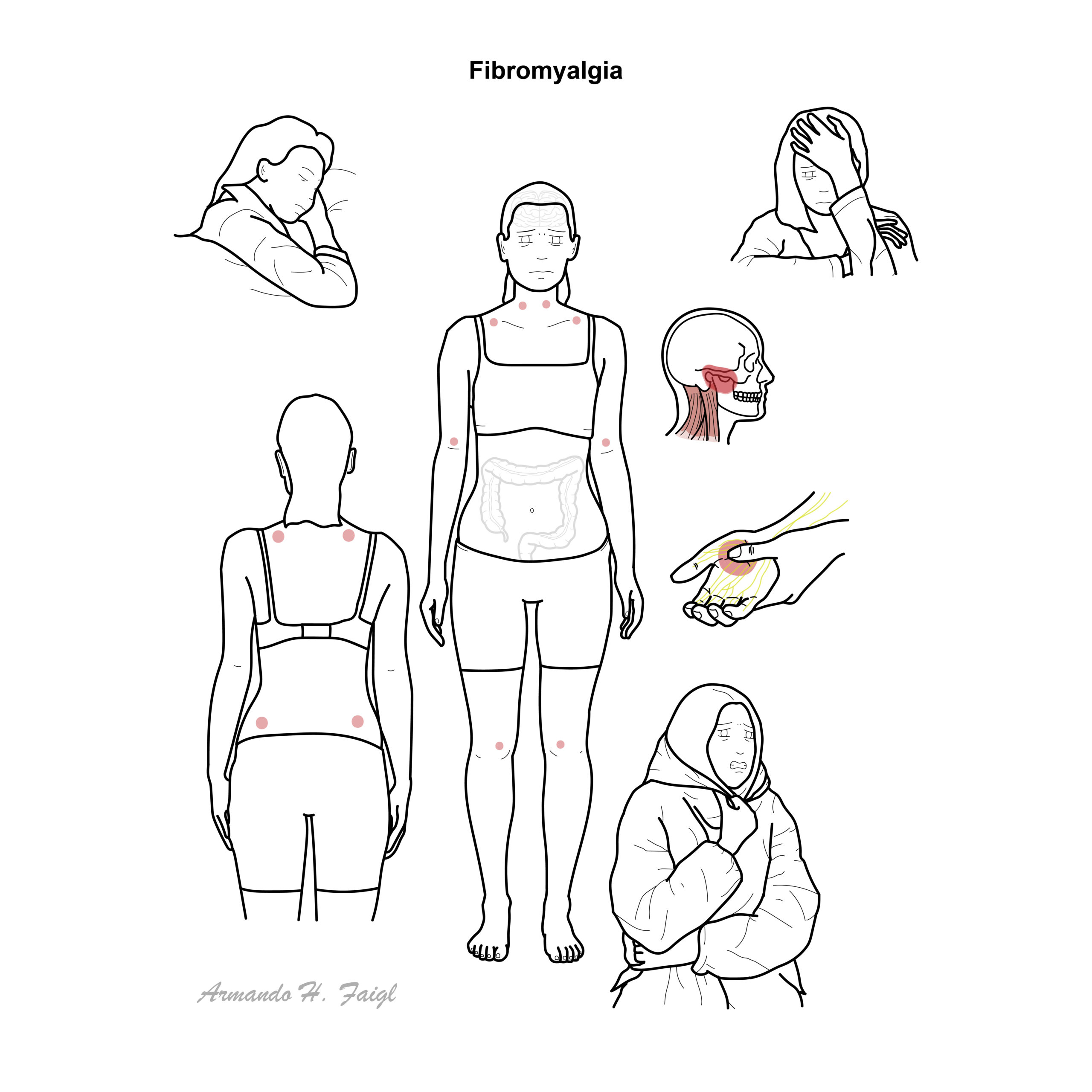
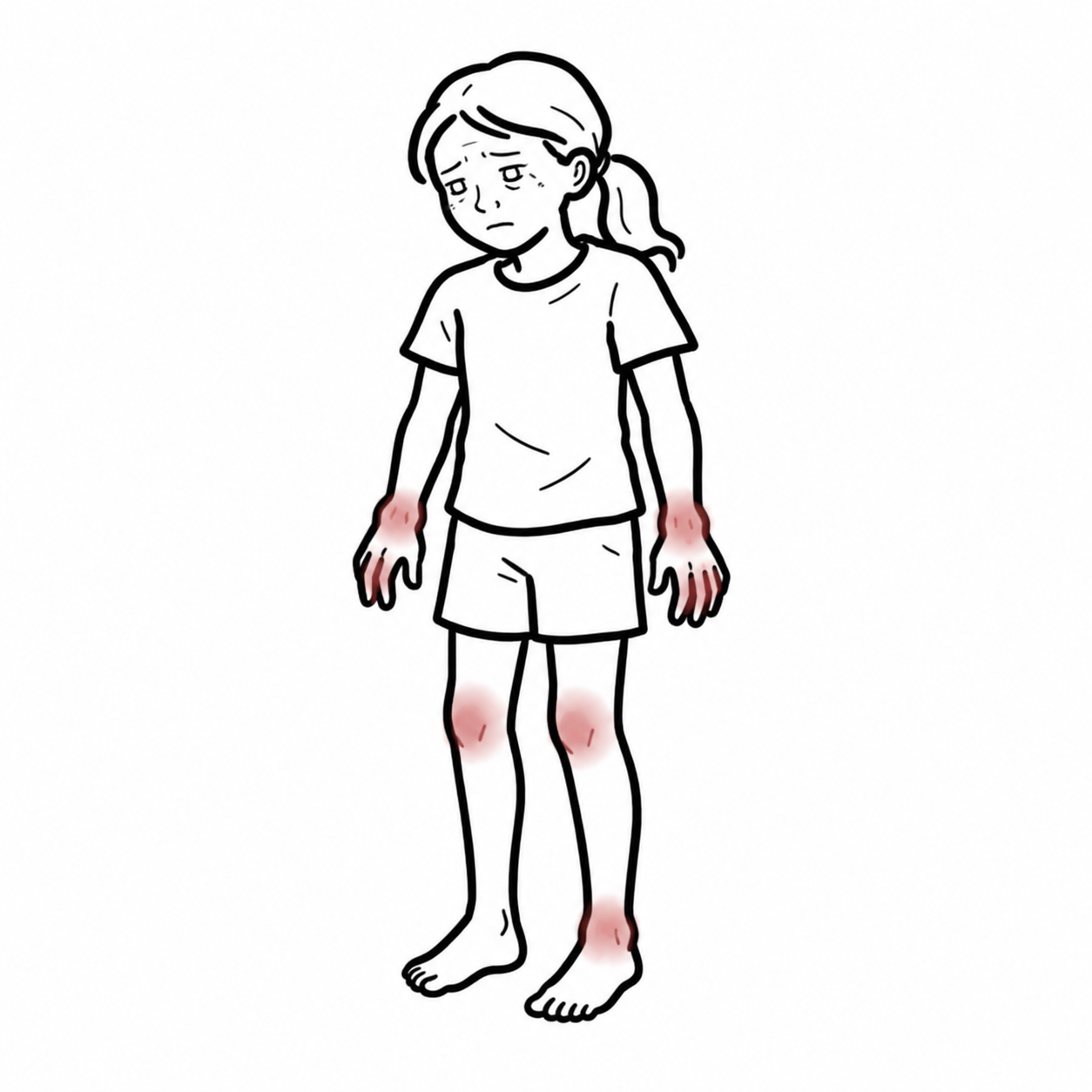
- Pain: chronic (≥3 months) widespread or multisite pain, often migratory; hyperalgesia/allodynia on light pressure (e.g., trapezius, lateral epicondyle, gluteal).
- Somatic symptoms: morning stiffness, paraesthesias, headaches/migraine, functional bowel/bladder symptoms, TMJ pain.
- Fatigue and post-exertional symptom exacerbation; non-restorative sleep, insomnia; cognitive “fibro-fog” (attention/processing speed).
- Mood: anxiety/depression common; heightened stress sensitivity.
- Autonomic: orthostatic intolerance, palpitations, thermodysregulation; sicca-like symptoms.
Clinical Examination
- Normal joints and neurology
- Tenderness to ~4 kg thumb pressure at multiple sites
- Normal ROM
- No synovitis
- No objective weakness.
Triad: Widespread pain + Fatigue + Non-restorative sleep.
Tender points are not required for diagnosis since 2010/2016 ACR criteria.
Diagnosis
- 2016 ACR Diagnostic Criteria:
- WPI ≥7 and SSS ≥5 or WPI 4–6 and SSS ≥9.
- Generalised pain in ≥4 of 5 regions (jaw, chest, abdomen excluded).
- Symptoms present at a similar level ≥3 months.
- Diagnosis valid irrespective of other illnesses if criteria met.
- AAPT 2019 criteria (alternative research/clinical framework): multisite pain (≥6/9 regions), fatigue and sleep/cognitive symptoms, ≥3 months, not better explained by another disorder.
- Investigations (rule-out/minimise over-testing): FBC, TSH, CRP/ESR, CMP ± CK, coeliac serology if GI symptoms; screen for OSA when indicated; consider B12, ferritin when fatigued; autoimmune tests only if clinical suspicion of CTD
- Differential Diagnosis
- Hypothyroidism (TSH ↑, cold intolerance).
- Inflammatory rheumatic disease (objective synovitis, raised CRP/ESR, erosions).
- Myopathies (objective weakness, CK ↑).
- Small fibre neuropathy (length-dependent burning pain, reduced IENFD on biopsy).
- Chronic fatigue syndrome/ME (post-exertional malaise predominates; overlapping but distinct).
Use the Polysymptomatic Distress (PSD) score (WPI+SSS) to track severity and response.
High patient-reported activity in RA/SLE with normal inflammatory markers often reflects coexistent fibromyalgia rather than uncontrolled inflammation 2,8.
FIBRO = Fatigue, Insomnia (non-restorative sleep), Brain-fog, Regional→widespread pain, Overdetection of pain (allodynia).
Treatment
- Conservative measures
- Education
- Graded aerobic/strength exercise (land or aquatic)
- CBT or psychologically informed therapy
- Prioritise sleep optimisation
- Self-management (pacing, goal setting)
- Adjuncts (individualise): meditative movement (tai chi, yoga), mindfulness-based stress reduction, acupuncture; treat comorbidities (depression, OSA, obesity) to improve global outcomes
- Pharmacological (for severe pain/sleep disturbance after core care)
- SNRIs: duloxetine or milnacipran (pain, function).
- Pregabalin (sleep, pain); gabapentin less certain.
- Low-dose amitriptyline/cyclobenzaprine mainly for sleep.
- Avoid routine NSAIDs, benzodiazepines, and avoid strong opioids (harms outweigh benefits); tramadol only as short-term rescue in select cases.
Care delivery: shared decision-making, explain nociplastic pain model, use PSD/Patient-Reported Outcomes to track progress; de-escalate ineffective drugs.
Exercise is the most consistently effective intervention across outcomes; start low, progress slow to avoid post-exertional flares.
If multiple drugs at moderate doses fail, re-build the non-drug plan (sleep, graded activity, CBT) rather than stacking medications.
Complications & Prognosis
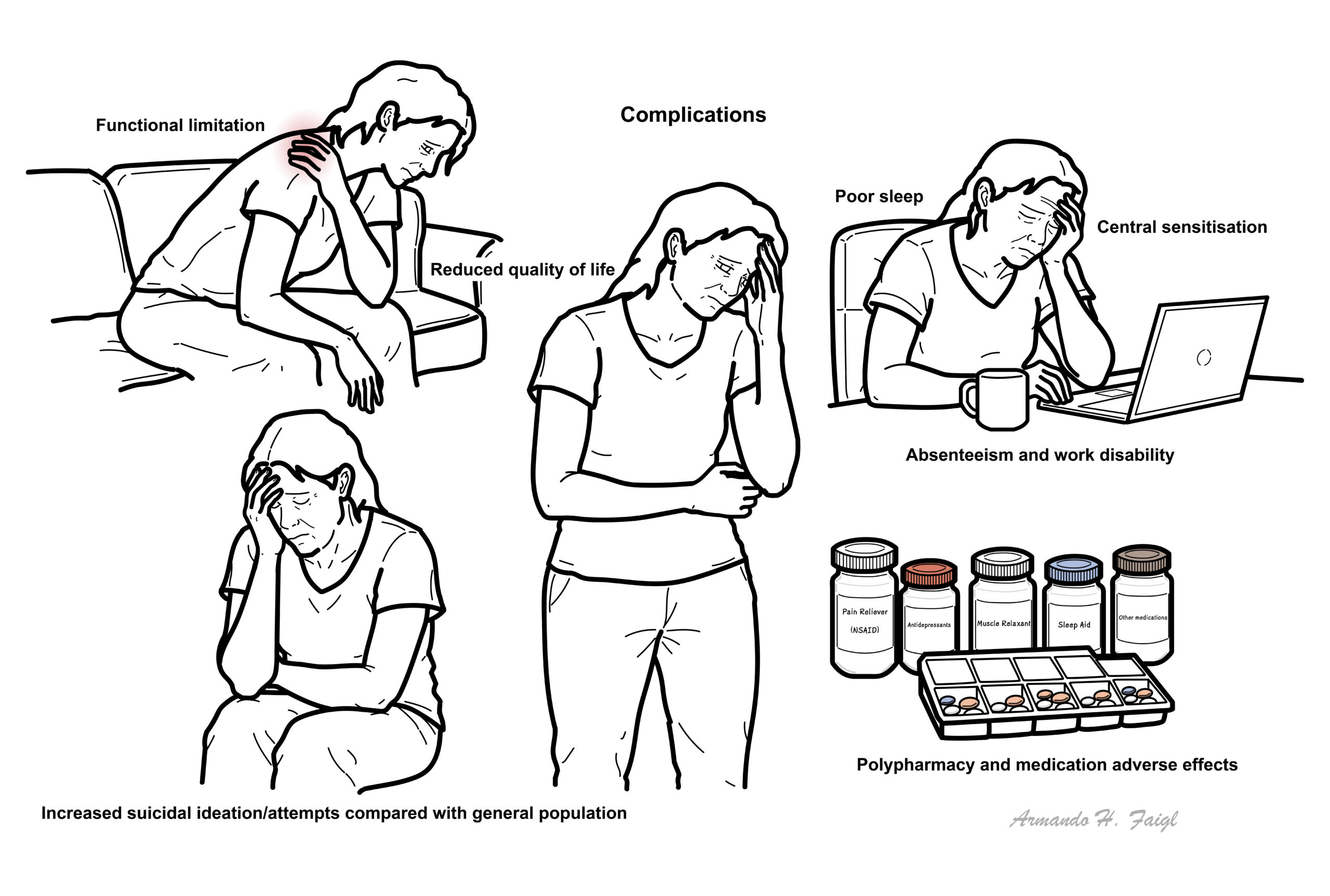
Complications
- Functional limitation
- Reduced QoL
- Absenteeism and work disability
- Polypharmacy
- Medication adverse effects
- Increased suicidal ideation/attempts compared with general population
- Fluctuating but modifiable course
- Many improve with non-pharmacological, multicomponent care
- Poorer prognosis with high baseline PSD, severe sleep disturbance, depression/anxiety, catastrophising, obesity, and persistent stressors 2,5.
Regular review to deprescribe ineffective agents and reinforce active strategies correlates with better long-term outcomes.
References
- Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319-329.
- Häuser W, Ablin J, Fitzcharles MA, et al. Fibromyalgia. Nat Rev Dis Primers. 2015;1:15022.
- Kosek E, Cohen M, Baron R, et al. Nociplastic pain: proposed criteria. Pain. 2021;162(11):2659-2664.
- Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Am J Phys Med Rehabil. 2016;95(9):S13-S23.
- Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR recommendations for the management of fibromyalgia: 2023 update. Ann Rheum Dis. 2023;82(9):1151-1162.
- Bidonde J, Busch AJ, Schachter CL, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst Rev. 2017;(6):CD012700.
- Bernardy K, Klose P, Welsch P, Häuser W. Efficacy of cognitive behavioural therapies in fibromyalgia: systematic review and meta-analysis. Schmerz. 2018;32(1):30-38.
- Fitzcharles MA, Nikiphorou E, Sedondi L, et al. Fibromyalgia and rheumatic diseases: diagnostic pitfalls and clinical impact. Best Pract Res Clin Rheumatol. 2019;33(3):101423.
- Grayston R, Czanner G, Elhadd K, et al. A systematic review and meta-analysis of small fiber pathology in fibromyalgia. Semin Arthritis Rheum. 2019;48(5):933-940.
- Albrecht DS, Forsberg A, Sandström A, et al. Brain glial activation in fibromyalgia — a [11C]-PBR28 PET study. Brain Behav Immun. 2019;75:72-83.
- Clauw DJ, Häuser W, Cohen SP, Fitzcharles MA. Considering the potential of centralised pain in primary care. Mayo Clin Proc. 2019;94(4):736-746.
- Arnold LM, Bennett RM, Crofford LJ, et al. AAPT Diagnostic Criteria for Fibromyalgia. Pain. 2019;160(9):1965-1973.
- Choy E. The role of sleep in pain and fibromyalgia. Nat Rev Rheumatol. 2015;11(9):513-520.
- Üçeyler N, Sommer C. Small fibre pathology in fibromyalgia: recent advances. Curr Opin Rheumatol. 2018;30(5):553-559.
- Løge-Hagen JS, Sæle A, Juhl C, et al. Suicidality in chronic pain and fibromyalgia: systematic review and meta-analysis. J Pain Res. 2017;10:2253-2263.








Members only discussions coming soon…