

Polymyalgia Rheumatica (PMR)

Overview
Polymyalgia rheumatica is a common inflammatory condition affecting older adults, typically over 50 years of age, characterised by pain and stiffness in the shoulder and pelvic girdles. It is strongly associated with elevated inflammatory markers and responds dramatically to low-dose corticosteroids. PMR is a clinical diagnosis and can mimic other rheumatic or non-rheumatic disorders. Importantly, PMR is closely linked to giant cell arteritis (GCA), which occurs in up to 15–20% of cases and must be actively screened for due to its risk of irreversible vision loss.
Definition
Polymyalgia: Generalised muscle pain affecting multiple areas, particularly the proximal limb girdles (shoulders, hips), without true myositis (normal CK).
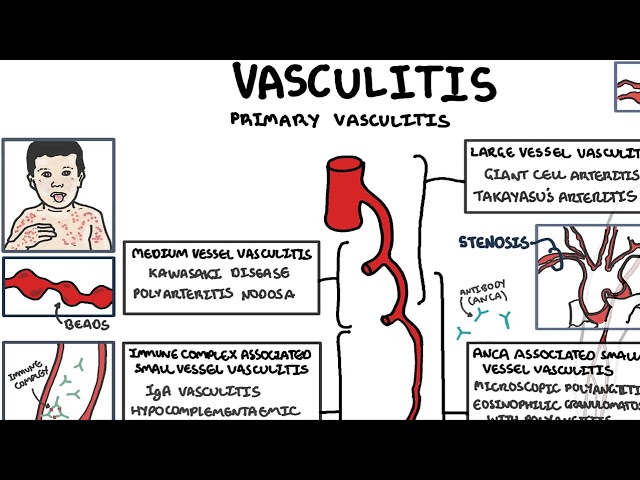
Giant Cell Arteritis: A large-vessel vasculitis associated with PMR. Presents with headache, jaw claudication, scalp tenderness, and vision loss. Requires urgent treatment with high-dose corticosteroids to prevent permanent blindness.
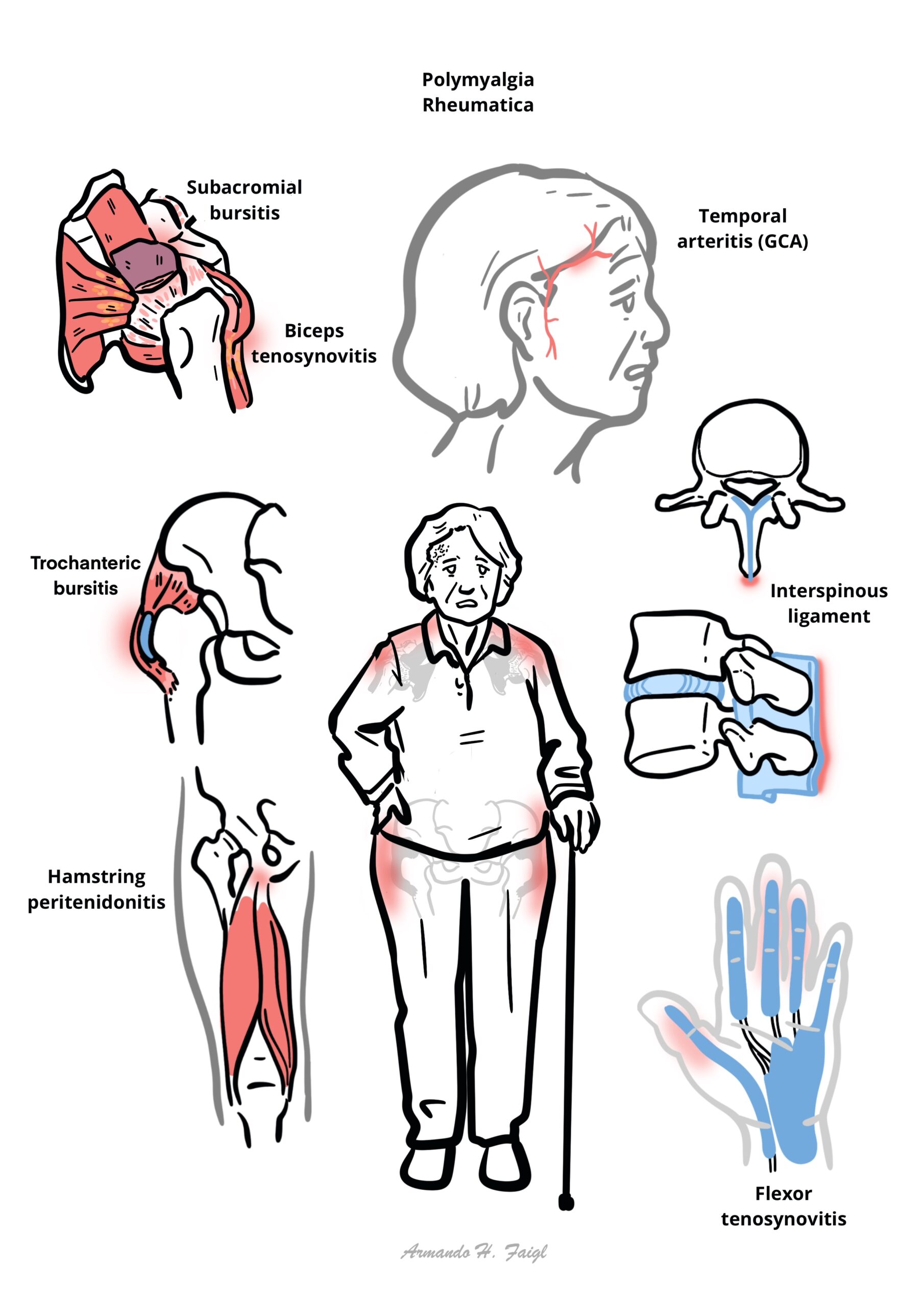
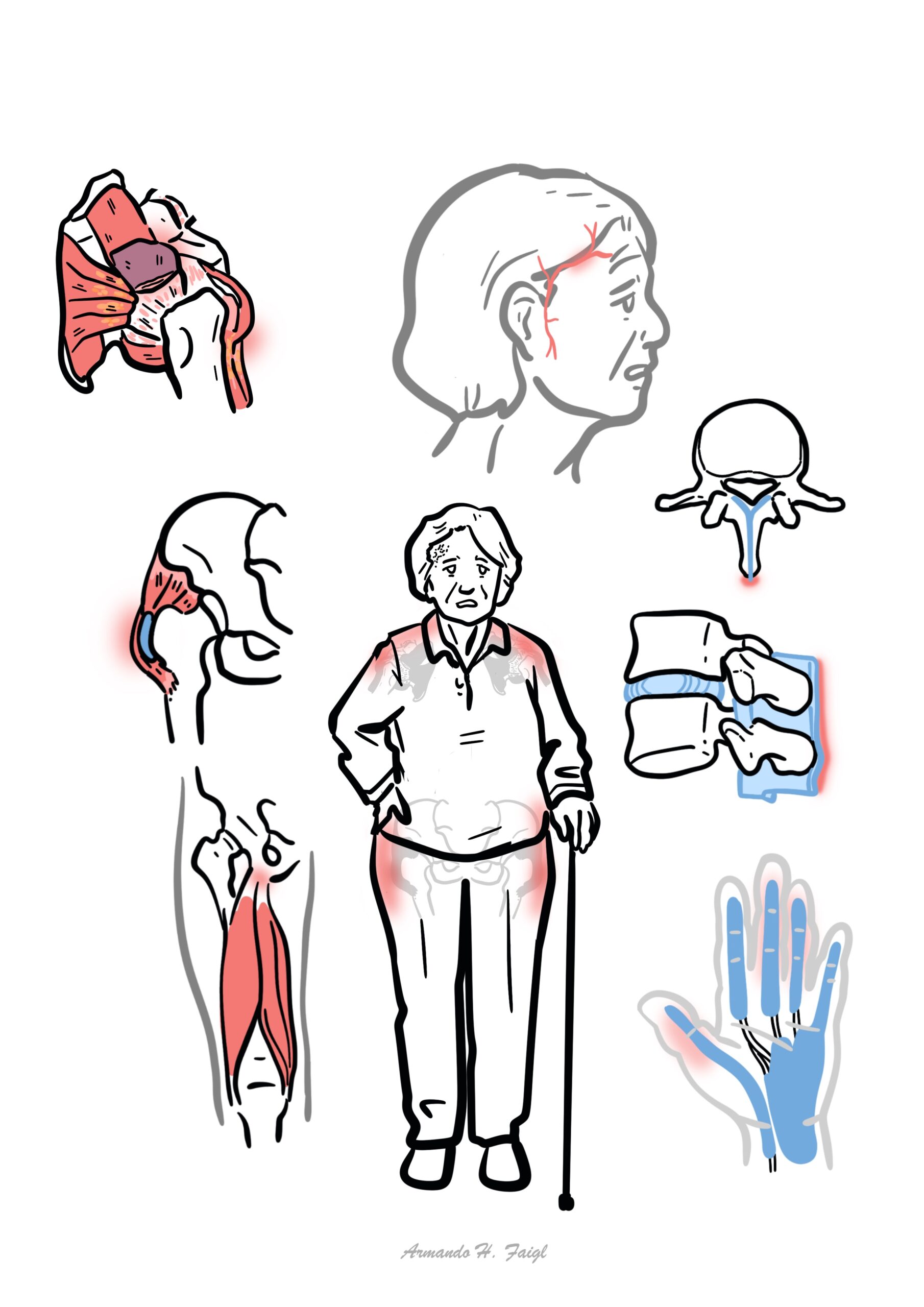
Anatomy & Physiology
- Targets periarticular structures (bursae, tendons, joint capsules), especially in shoulders and hips.
- Muscles are clinically tender but not inflamed (normal muscle biopsy and CK).
- Pain and stiffness arise from synovitis and bursitis, not from myopathy.
Aetiology & Risk Factors
- Unknown aetiology, but likely autoimmune with environmental triggers.
- Risk factors:
- Age >50 years
- Female sex
- Northern European descent
- Genetic predisposition: HLA-DR4
- Seasonal variation (suggests infectious trigger)
Pathophysiology
- Likely autoimmune process, with T-cell activation and cytokine release (IL-6, IL-1β, TNF-α).
- Inflammation mainly affects the structures around the joint; bursae, tendons
- Associated with GCA, suggesting a shared pathogenesis involving large-vessel vasculitis.
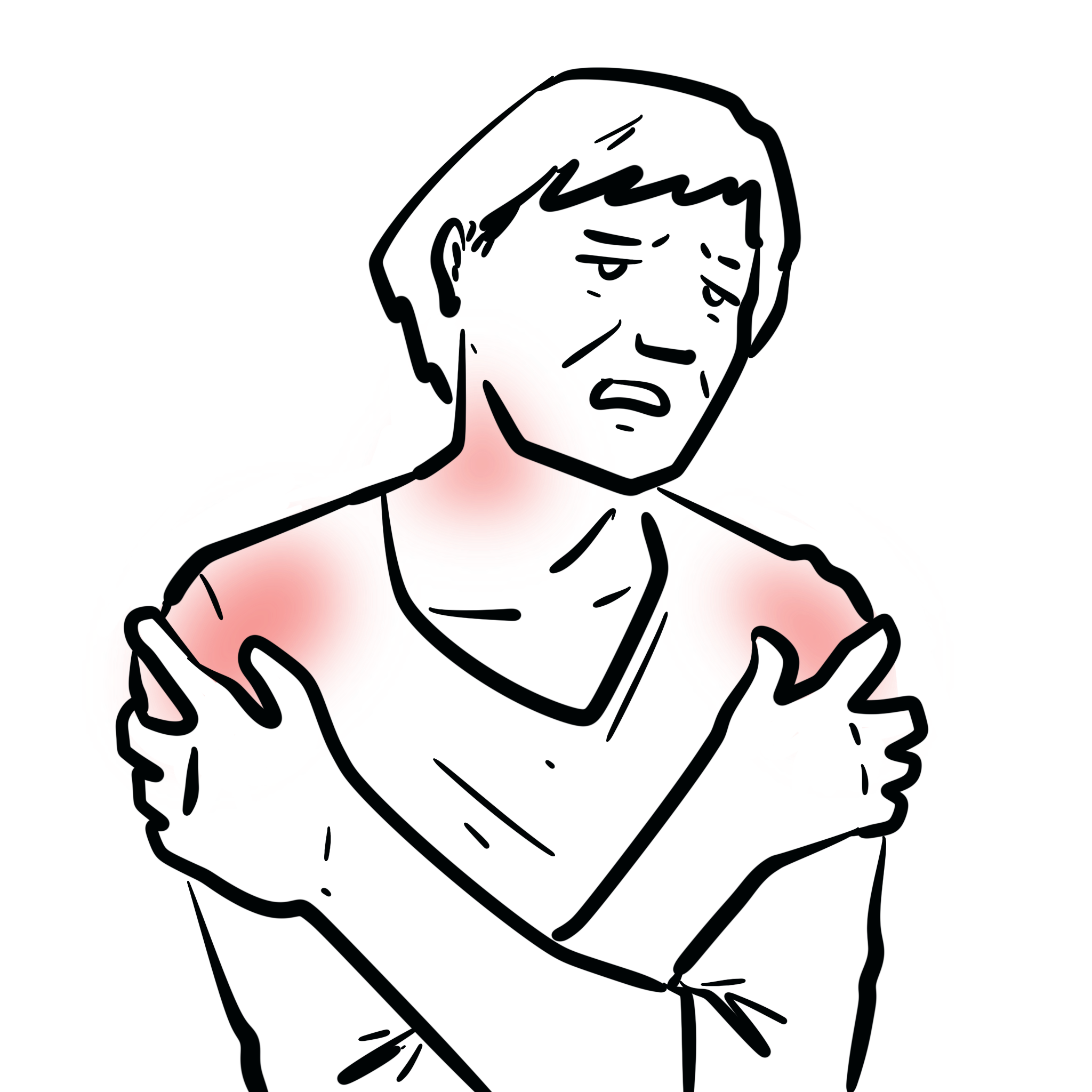
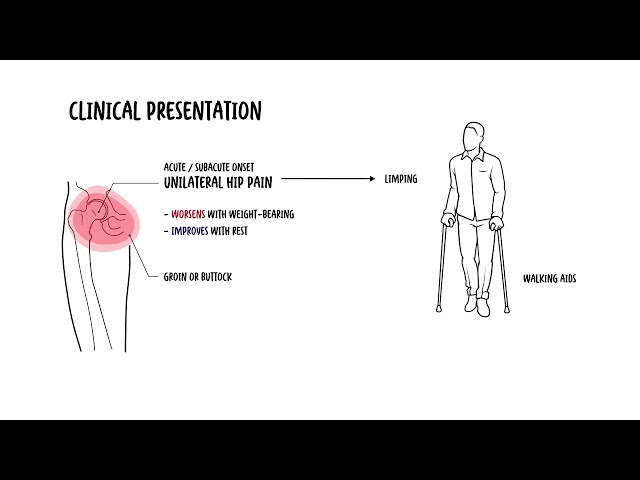
Clinical Manifestations
If an elderly patient presents with bilateral shoulder pain and morning stiffness with high CRP — think PMR before jumping to frozen shoulder or osteoarthritis.
- Bilateral shoulder pain (most common initial symptom)
- Hip girdle pain/lower back pain
- Posterior knee pain
- Morning stiffness >45 minutes
- Carpal tunnel syndrome
- Functional limitation: difficulty rising from chair, lifting arms, dressing
- Systemic symptoms:
- Fatigue
- Weight loss
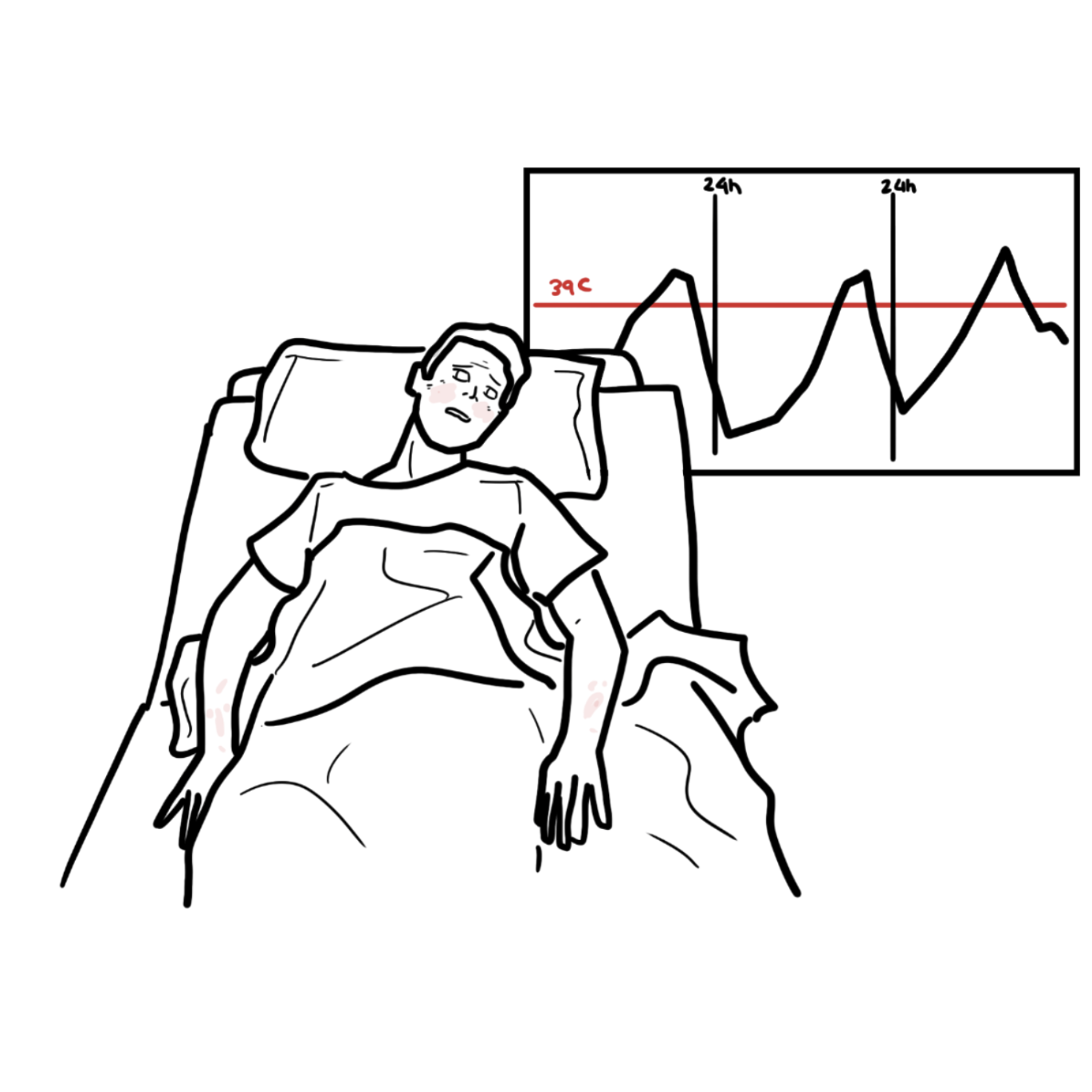
- Low-grade fever
- Depression
Muscle strength is normal on examination, though movement is limited by pain.
Always ask about GCA, and investigate especially if new headache, jaw claudication, or visual symptoms.
Diagnosis
- Clinical diagnosis based on history, exam, and response to steroids.
- Investigations:
- ↑ ESR (>40 mm/hr) and/or ↑ CRP
- Normocytic anaemia, thrombocytosis
- Normal CK, TSH (to exclude hypothyroid myopathy)
- Rule out infection, malignancy, RA, myositis
- Imaging:
- US or MRI: subacromial/subdeltoid bursitis, hip synovitis
Normal CK helps distinguish PMR from inflammatory myopathies.
Diagnostic Criteria (EULAR/ACR 2012):
- Age ≥50 years
- Bilateral shoulder pain
- Abnormal CRP and/or ESR
- Morning stiffness >45 mins
- New hip pain
- No RF or anti-CCP
- Absence of peripheral synovitis
Classification
- Typical PMR: classic symptoms, normal CK, good steroid response
- PMR-like syndrome: seen with paraneoplastic syndromes or other inflammatory diseases (e.g. RA)
Treatment
- Prednisone 12.5–25 mg daily, with rapid response in 24–72 hours
- Taper slowly over 12–18 months
- Monitor inflammatory markers and symptoms
- Consider methotrexate in relapsing cases or steroid-sparing strategy
- Consider IL6 inhibitors
- Consider also JAKi
- Monitor for side effects of corticosteroids
Rapid improvement within 24 hours of low-dose steroids is both diagnostic and therapeutic.
Lack of response to steroids should prompt reconsideration of diagnosis. Consider PET-CT if atypical symptoms or poor response to therapy — may reveal underlying vasculitis or malignancy.
Complications and Prognosis
- Relapse (30–50%): typically during taper
- Steroid-related: osteoporosis, diabetes, hypertension, cataracts
- Misdiagnosis: important to exclude mimics (malignancy, myositis)
- Undetected GCA → visual loss
- Good with appropriate treatment
- Most patients can stop steroids within 2 years
- Does not cause joint erosion or deformity
Giant Cell Arteritis (GCA)
- Occurs in 15–20% of PMR cases
- Large-vessel vasculitis affecting temporal arteries and aorta
- Symptoms:
- New-onset headache
- Scalp tenderness
- Jaw claudication
- Vision changes or loss
- Systemic symptoms (fever, weight loss)
- Diagnosis: temporal artery biopsy, raised ESR/CRP, imaging (e.g. Ultrasound, PET-CT)
- Treatment: high-dose prednisone (40–60 mg/day) urgently to prevent blindness then aim for Tocilizumab (IL-6)
PMR-Onset Rheumatoid Arthritis
- PMR-onset RA should be suspected in patients with persistent synovitis, especially of the wrists, MCPs, or knees, which is not typical of classic PMR.
- A partial or poor response to low-dose corticosteroids suggests the possibility of evolving RA rather than isolated PMR.
- RF or anti-CCP usually negative (seronegative RA) but if positive supports diagnosis.
- Radiographic erosions are not seen in PMR — their presence points toward RA.
- Elderly-onset RA may be seronegative and mimic PMR, requiring close follow-up.
References
- Dasgupta B, Cimmino MA, Maradit-Kremers H, et al. 2012 Provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Arthritis Rheum. 2012;64(4):943–954.
- González-Gay MA, Matteson EL, Castañeda S. Polymyalgia rheumatica. Lancet. 2017;390(10103):1700–1712.
- Dejaco C, Singh YP, Perel P, et al. 2015 Recommendations for the management of polymyalgia rheumatica: a EULAR/ACR guideline. Ann Rheum Dis. 2015;74(10):1799–1807.
- Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. N Engl J Med. 2002;347(4):261–271.







Members only discussions coming soon…