Liver Mass I Tumour


Author
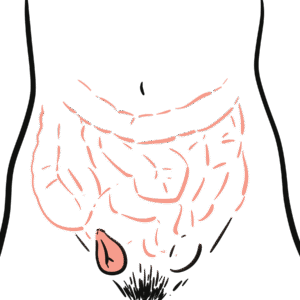
Liver tumors are divided into Benign and Malignant. Most liver tumors are benign, asymptomatic and found incidentally on unrelated imaging. Malignant liver tumours are associated with risk factors (Hep C, Cirrhosis) and present with a spectrum of clinical signs and symptoms such as right upper quadrant pain and liver failure.
Hepatic Adenoma: benign epithelial tumors of hepatocytes
Hepatic Carcinoma: primary malignant tumors of hepatocytes
Cirrhosis: morphological change in liver parenchyma as a result of chronic liver disease triggering an inflammatory response, characterized by fibrosis and regenerative nodules.
Is the most common liver tumor in young women who have a history of sex hormone use( oral contraceptives, anabolic steroids ) with the most common symptom being right abdominal pain.
Pain is caused by the mass pressing against the liver capsule or as a result of hemorrhagic necrosis as blood supply is compressed.
Hepatic adenomas have tendency to rupture which leads to life threatening intra abdominal bleeding.
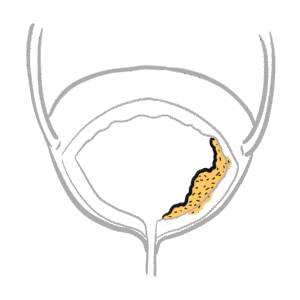
It is important to distinguish it from other benign lesions as it has malignant potential. It is usually located in the right lobe of the liver and seen as round, well defined ,well circumscribed mass with yellow discoloration due to abundance of fat.
Usually as treated by surgical resection (tumors more than 5cm) but in cases where mass is too small sex hormone use is withdrawn.
Biopsy is contraindicated as it may cause bleeding.
Develop in response to liver injury and are comprised of a proliferation of hepatocytes and surrounding stroma. They are typically seen in the setting of cirrhosis
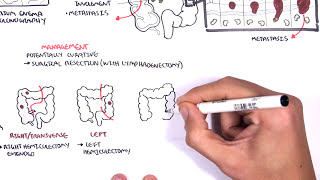
Most malignant tumours of the liver are metastatic (from pancreas, colon, stomach, breast)
Are the most common primary liver tumours with a background of chronic liver disease such as cirrhosis and hepatitis. Arises from liver parenchymal cells.
Aspergillus is found in staple food crops of Asia and Africa such as corn ,rice and nuts.
Clinical presentation is variable, it is masked by underlying cirrhosis or hepatitis in cases caused by these diseases. Commonly presents with rapid deterioration in pre-existing cirrhosis. Where aflatoxin may be the risk factor patients may present with abdominal fullness, upper abdominal pain, malaise, weight loss ,and jaundice.
Liver function tests maybe be elevated ,serum alpha-fetoprotein maybe elevated but is mainly associated with advanced HCC. Ultrasound is performed to confirm mass. Further imaging studies (CT,MRI) are performed to confirm the diagnosis.
Intrahepatic metastases by either vascular invasion or direct extension become more likely once tumors reach 3 cm in size.
The 5-year survival of large tumors is dismal, and the majority of patients die within 2 years of diagnosis. Tumors that are resected at less than 3cm may increase survival to 3 years.
Targeted medications include atezolizumab/bevacizumab and sorafenib.
Are the second most common malignancy of the liver which affects the bile ducts. Arises in the extrahepatic biliary tree, but may be intrahepatic. Its classified according to its anatomical location
All these risk factors cause chronic inflammation and cholestasis, which are thought to promote mutations and epigenetic changes.
Postoperative complications include:
5 year survival rate is 30% following surgery.











Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion