

Non-Hodgkins Lymphoma
Overview
Non-Hodgkin lymphoma (NHL) is a heterogeneous group of lymphoid malignancies arising from B cells, T cells, or natural killer (NK) cells, characterised by clonal proliferation of lymphocytes at different stages of differentiation. It accounts for approximately 4–5% of all cancers worldwide, with incidence increasing with age and a median diagnosis in the sixth to seventh decade. B-cell lymphomas represent ~85–90% of cases. NHL encompasses a wide clinical spectrum from indolent (e.g., follicular lymphoma) to aggressive (e.g., diffuse large B-cell lymphoma) and highly aggressive subtypes (e.g., Burkitt lymphoma). Risk factors include immunosuppression, infections (EBV, H. pylori, HIV), autoimmune disease, and environmental exposures.
Definition
Lymphoma: Malignancy of lymphocytes arising from lymphoid tissues.
Non-Hodgkin lymphoma: Group of lymphoid malignancies excluding Hodgkin lymphoma, lacking Reed-Sternberg cells.
B-cell lymphoma: Malignancy derived from B lymphocytes (~85–90% of NHL).
Indolent vs aggressive lymphoma: Classification based on growth rate and clinical behaviour.
NHL is a spectrum of diseases, not a single entity.
Anatomy & Physiology
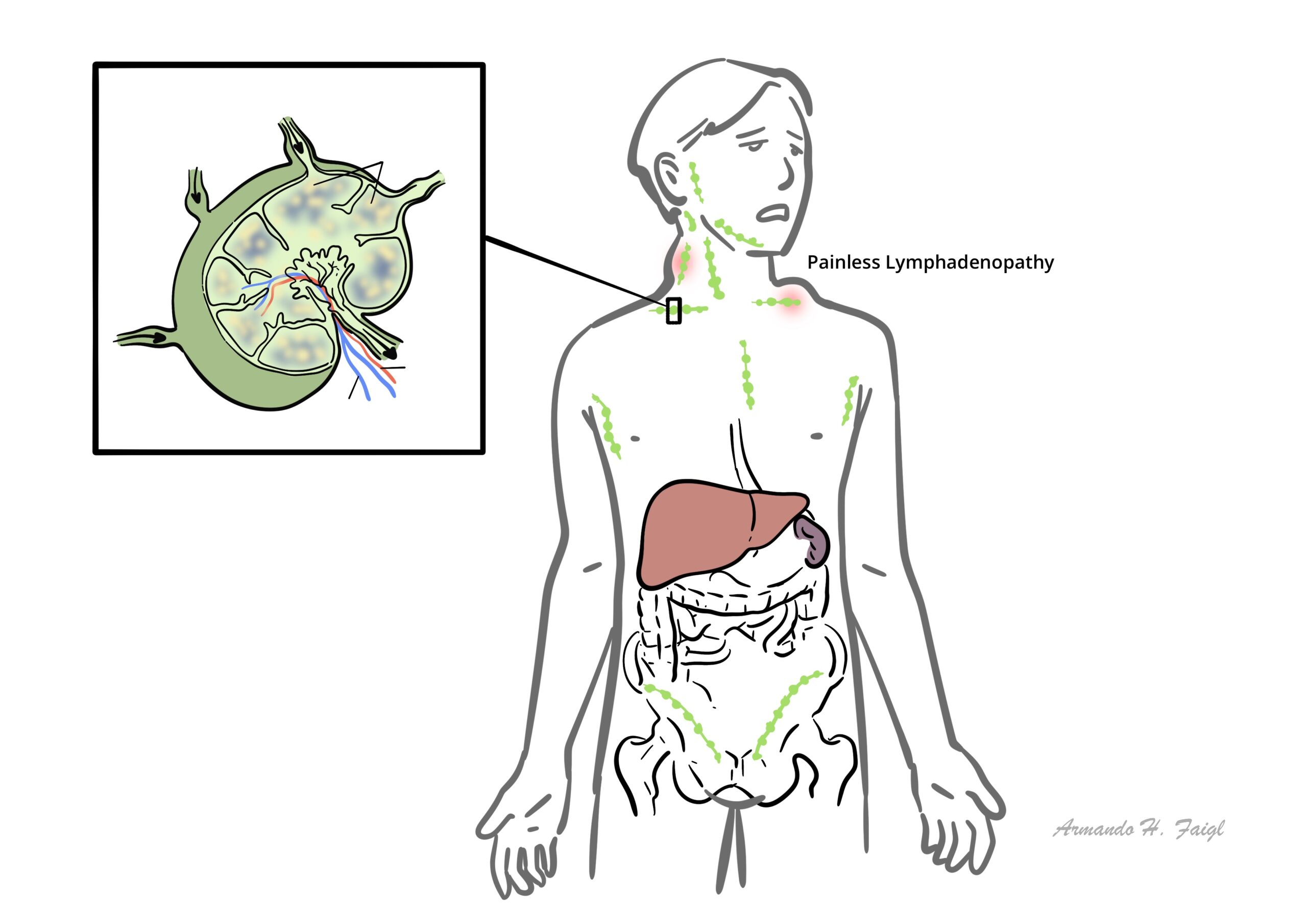
- Lymphatic system: Network of lymph nodes, spleen, thymus, and lymphatic vessels responsible for immune surveillance
- Lymph node structure: Cortex (B-cell follicles), paracortex (T-cells), medulla (plasma cells, macrophages)
- B-cell maturation: Occurs in bone marrow → germinal centre reaction → antibody production
- T-cell function: Cell-mediated immunity, immune regulation
Aetiology & Risk Factors
Aetiology
- Genetic mutations (e.g., BCL2, MYC, BCL6 rearrangements)
- Chronic antigenic stimulation
- Viral oncogenesis
- Immunosuppression (HIV, post-transplant)
- Infections: EBV, H. pylori, HTLV-1, hepatitis C
- Autoimmune diseases (RA, Sjögren’s)
- Environmental exposures (radiation, chemicals)
- Increasing age
Chronic immune stimulation → increased risk of malignant transformation.
Pathophysiology
- Genetic mutation in lymphocyte → clonal expansion
- Dysregulated apoptosis (e.g., BCL2 overexpression)
- Accumulation in lymph nodes and extranodal tissues
- Disruption of normal immune function
- Bone marrow infiltration → cytopenias
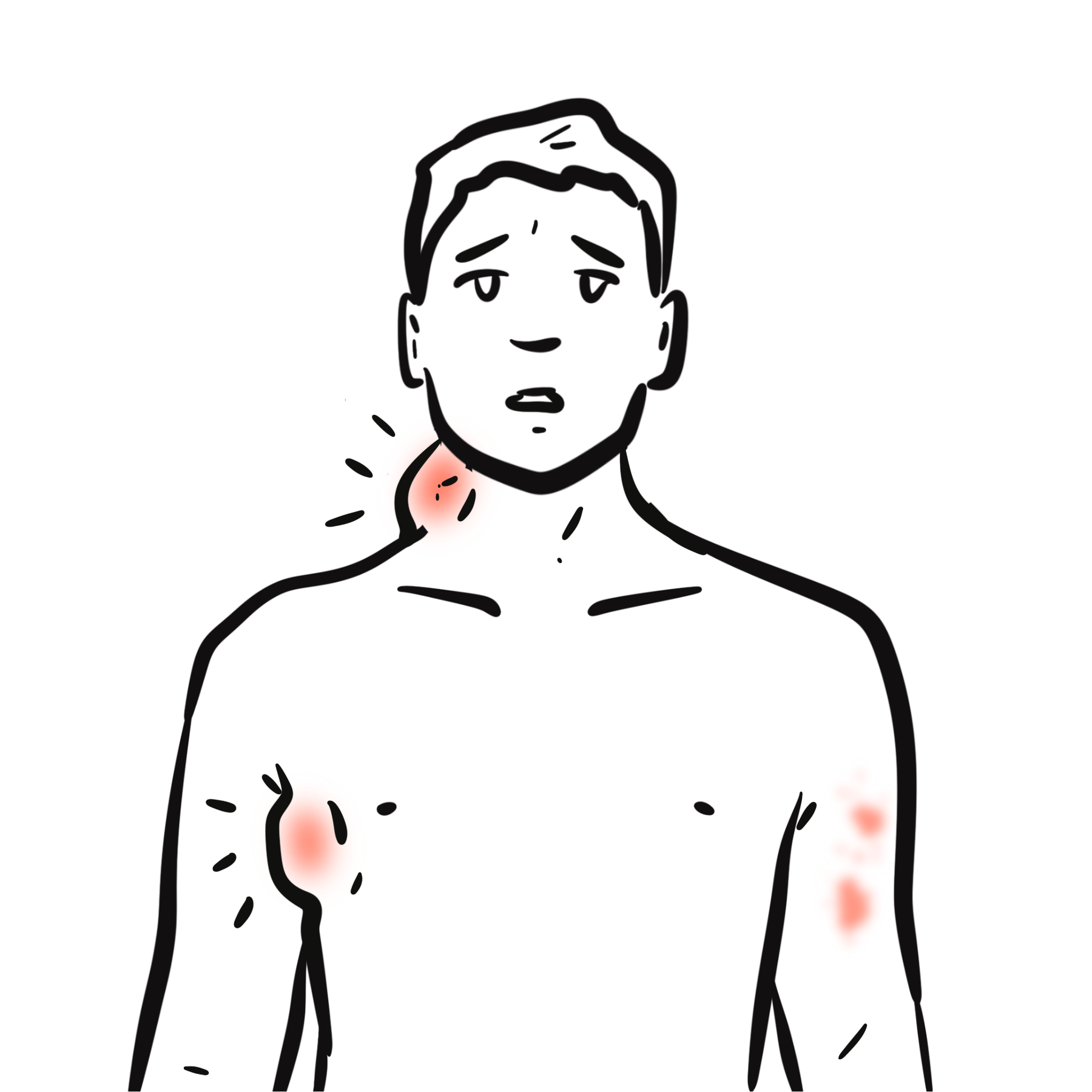
Clinical Manifestations
- Painless, firm lymphadenopathy
- B symptoms:
- Fatigue and malaise
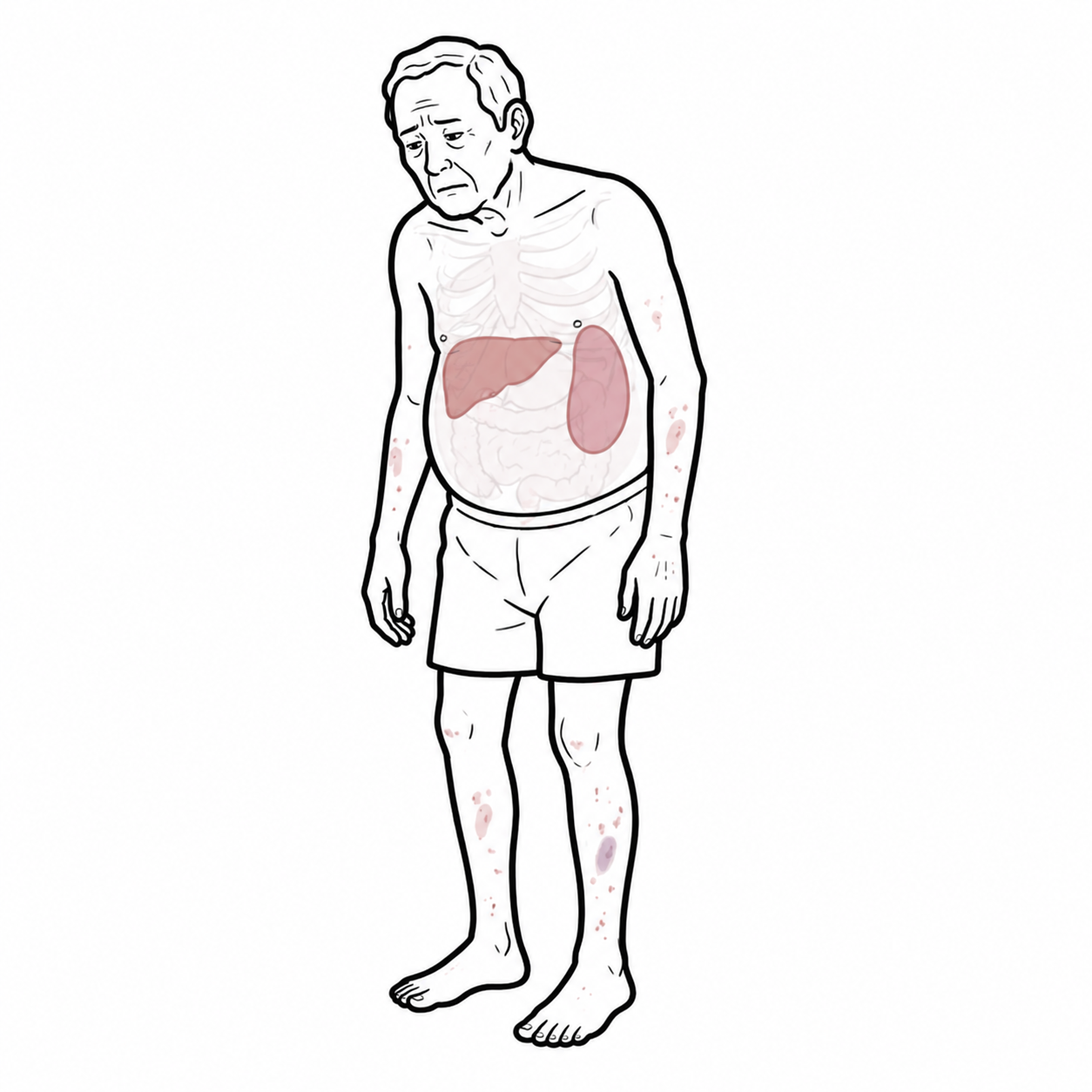
- Splenomegaly or hepatomegaly
- Extranodal disease:
- GI tract → abdominal pain, bleeding, obstruction
- CNS → headache, seizures, neurological deficits
- Skin → rash, nodules or plaques
- Testes → painless swelling
- Compression symptoms from bulky lymphadenopathy
- Mediastinal mass → cough, dyspnoea, chest discomfort
- Superior vena cava obstruction → facial swelling, venous distension
- Abdominal/pelvic nodes → abdominal pain, bowel or urinary obstruction
- Symptoms may vary by subtype
Non-Hodgkin lymphoma is more likely than Hodgkin lymphoma to present with extranodal involvement and can have a very variable clinical presentation.
Diagnosis
Diagnostic Criteria (WHO classification 2016+ / ICC 2022):
- Histopathological confirmation required
- Immunophenotyping + molecular classification essential
- Excisional lymph node biopsy (gold standard)
- Immunohistochemistry (CD markers)
- Flow cytometry
- PET-CT for staging
- Bone marrow biopsy
- Blood tests: LDH, FBC
- Hodgkin lymphoma
- Reactive lymphadenopathy
- Leukemia
Excisional biopsy > FNA. Excisional biopsy is preferred over FNA in suspected lymphoma because it preserves lymph node architecture, enabling accurate classification and definitive diagnosis.
Classification
By Cell Type:
- B-cell lymphomas
- T-cell/NK-cell lymphomas
By Behaviour:
- Indolent (slow-growing)
- Aggressive
- Highly aggressive
Table – Common Subtypes
| Subtype | Behaviour | Key Feature |
| DLBCL | Aggressive | Most common NHL |
| Follicular lymphoma | Indolent | t(14;18), BCL2 |
| Burkitt lymphoma | Highly aggressive | MYC translocation |
| Mantle cell lymphoma | Aggressive | Cyclin D1 overexpression |
Treatment
Treatment depends on type of NHL and disease burden
- Chemotherapy: R-CHOP = rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone.
- Adjuncts
- Methotrexate (CNS prophylaxis)
- Mesna (high dose cyclophosphamide or ifosfamide are at risk of haemorrhagic cystitis)
- Radiotherapy
- Targeted therapy (BTK inhibitors, CAR-T)
- Stem cell transplant (selected patients)
Always assess risk of tumour lysis syndrome, infection, hepatitis B reactivation, fertility issues, and cardiac function before treatment.
Rituximab is used for CD20-positive B-cell lymphomas.
R-CHOP = rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone.
| Treatment Overview | |
| NHL type | Usual first-line approach |
| Diffuse large B-cell lymphoma (DLBCL) | R-CHOP or similar chemoimmunotherapy; aggressive but potentially curable |
| Follicular lymphoma, asymptomatic low burden | Watch and wait |
| Follicular lymphoma, symptomatic/high burden | Anti-CD20 therapy ± chemotherapy, e.g. rituximab-based treatment |
| Burkitt lymphoma | Urgent intensive multi-agent chemotherapy + CNS prophylaxis |
| Mantle cell lymphoma | Immunochemotherapy ± BTK inhibitor; transplant considered in fit younger patients |
| Marginal zone lymphoma | Treat cause if present, e.g. H. pylori eradication in gastric MALT; radiotherapy or rituximab-based therapy if persistent/disseminated |
| Relapsed/refractory aggressive B-cell NHL | Salvage therapy, CAR-T, bispecific antibodies, or transplant depending on fitness and prior response |
Complications & Prognosis
- Bone marrow failure
- Infections
- Tumour lysis syndrome
- CNS involvement
- Variable depending on subtype
- Indolent lymphomas: long survival, often incurable
- Aggressive lymphomas: potentially curable
- Poor prognostic factors:
- Age
- Elevated LDH
- Advanced stage
- Poor performance status
References
- Swerdlow SH, et al. WHO classification of lymphoid neoplasms. Blood. 2016.
- Armitage JO. The aggressive non-Hodgkin lymphomas. N Engl J Med. 2018.
- NCCN Guidelines for Non-Hodgkin Lymphoma. 2024.
- Tilly H, et al. Diffuse large B-cell lymphoma. Lancet. 2015.
- National Cancer Institute. NHL overview. 2023.



Members only discussions coming soon…