

Vitamin B12 Deficiency Anaemia
Overview
Vitamin B12 (cobalamin) deficiency is a common cause of megaloblastic anemia, a variety of neuropsychiatric symptoms, and elevated serum homocysteine levels, especially in older persons. The recognition and treatment of vitamin B12 deficiency is critical since it is a reversible cause of bone marrow failure and demyelinating nervous system disease.
Definition
Anaemia (Anemia): The World Health Organization defines anaemia as a haemoglobin (Hb) concentration below 13 g/dl (130 g/L) in men over 15 years of age, below 12 g/dl (120g/L) in non-pregnant women over 15 years of age, and below 11 g/dl (110g/L) in pregnant women
Iron deficiency anaemia: Most common type of anemia, and it occurs when your body doesn’t have enough of the mineral iron
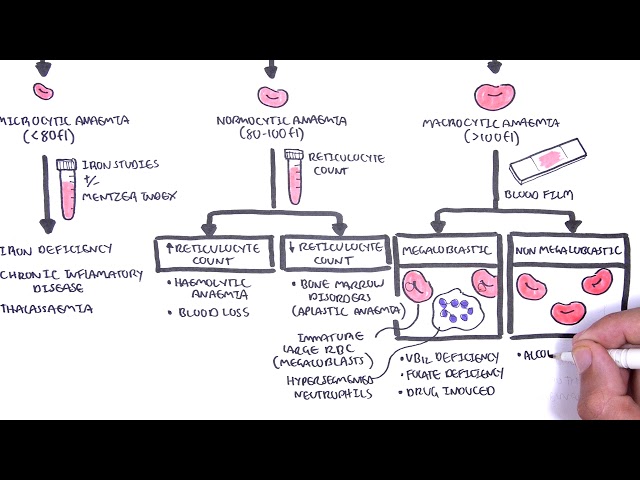
Microcytic anemia Defined as the presence of small, often hypochromic, red blood cells in a peripheral blood smear and is usually characterized by a low mean cell volume (MCV) (<83 micron3). Iron deficiency is the most common cause of microcytic anemia.
Normocytic anaemia: defined by a normal mean corpuscular volume (MCV), but the hemoglobin and hematocrit are decreased. Usually a result of hemolytic anaemia or anaemia of chronic disease
Mactocytic anaemia (Macrocytosis): defined as a mean corpuscular volume greater than 100 fL, is frequently encountered when a complete blood count is performed. The most common etiologies are alcoholism, vitamin B12 and folate deficiencies, and medications.
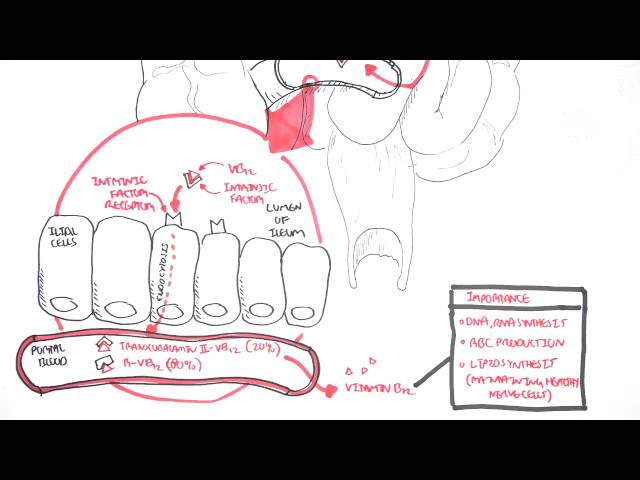
Physiology of Vitamin B12 digestion and Abosorption
Vitamin B12 is found in meat, fish, and dairy products. NOT in plants. The liver can store Vitamin B12 and stores are sufficient for up to 5 years. The daily requirement of vitamin B12 is about 2.4 μg.
Vitamin B12 is found almost exclusively in animal-based foods and is therefore a nutrient of potential concern for those following a vegetarian or vegan diet. Vegans, and anyone who significantly limits intake of animal-based foods, require vitamin B12-fortified foods or supplements.
Vitamin B12 (cobalamin) is a water-soluble vitamin that is crucial to normal neurologic function, red blood cell production, and DNA synthesis.
Aetiology and Risk Factors
Aetiology
- Pernicious anemia (autoimmune-mediated chronic atrophic gastritis) – most common cause of severe vitmain b12 deficiency
- Postsurgical malabsorption
- Dietary deficiencies
- Vitamin B12malabsorption from food
Decreased ileal absorption
- Crohn’s disease
- Ileal resection
- Tapeworm infestation
Decreased intrinsic factor
- Atrophic gastritis
- Pernicious anaemia
- Postgastrectomy syndrome
Genetic
- Transcobalamin II deficiency
Inadequate intake
- Alcohol abuse
- Older persons
- Vegetarians
Prolonged medication use
- Metformin
- Proton pump inhibitors
- Histamine h2 blockers
Clinical Manifestation
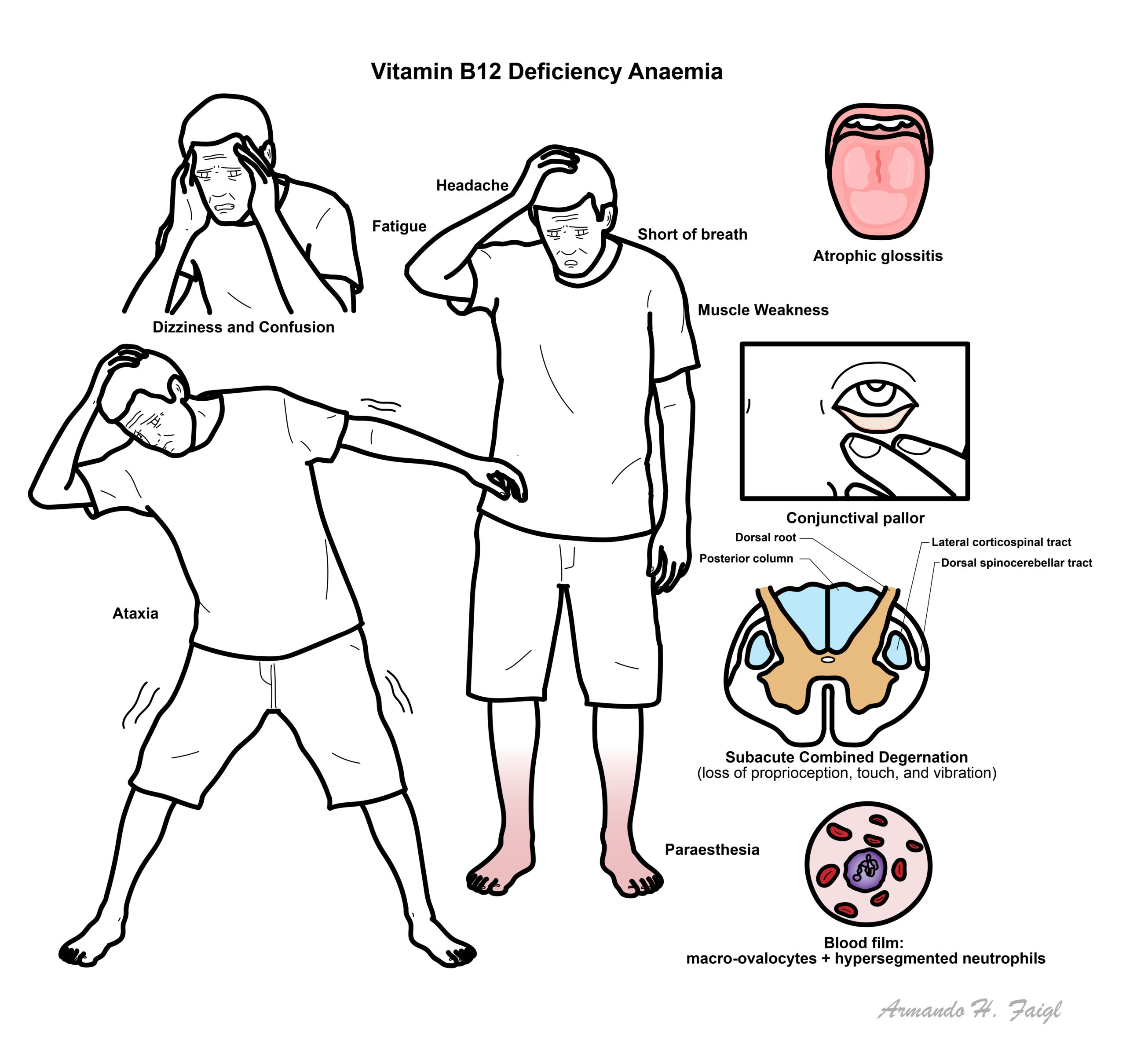
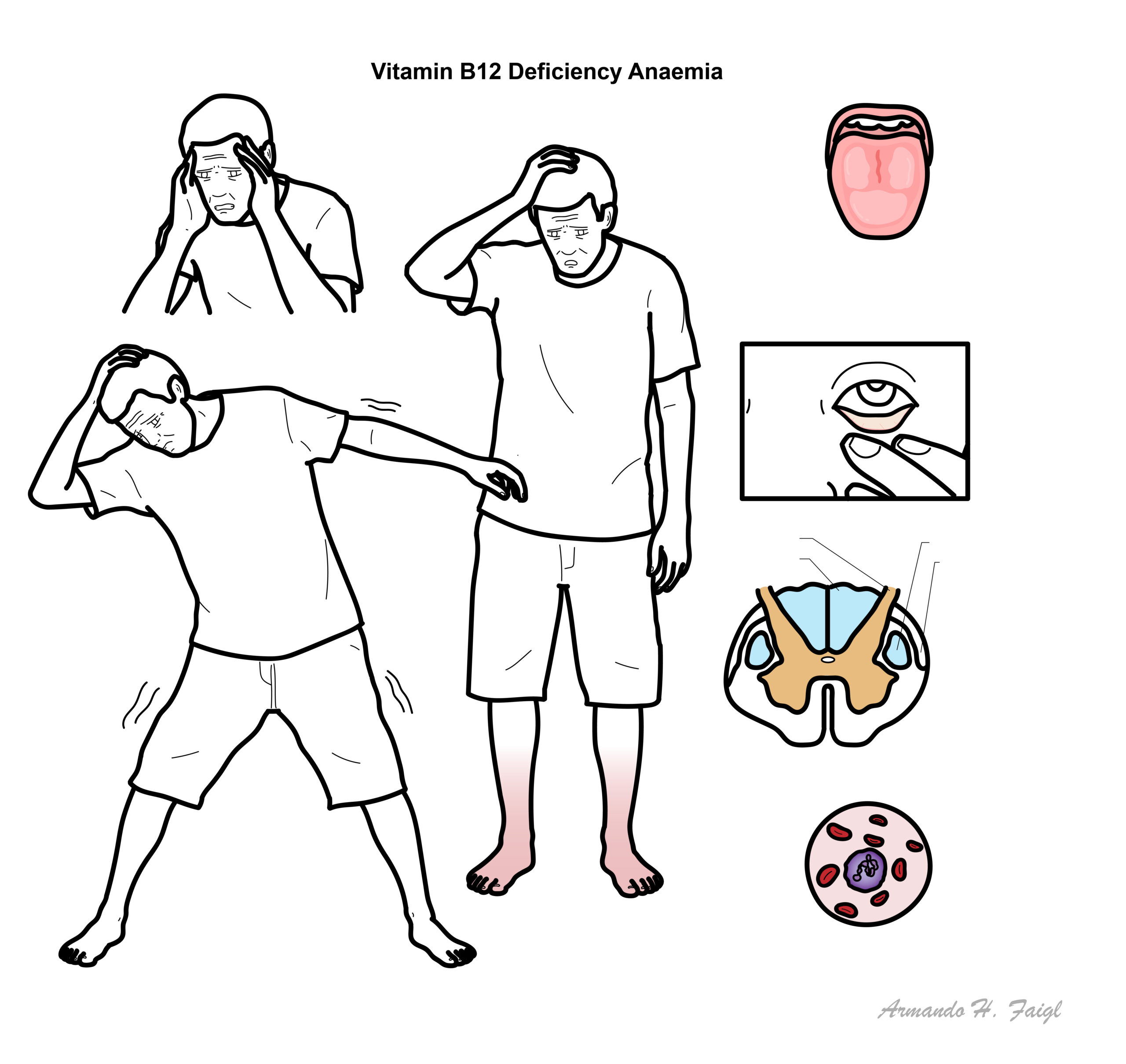
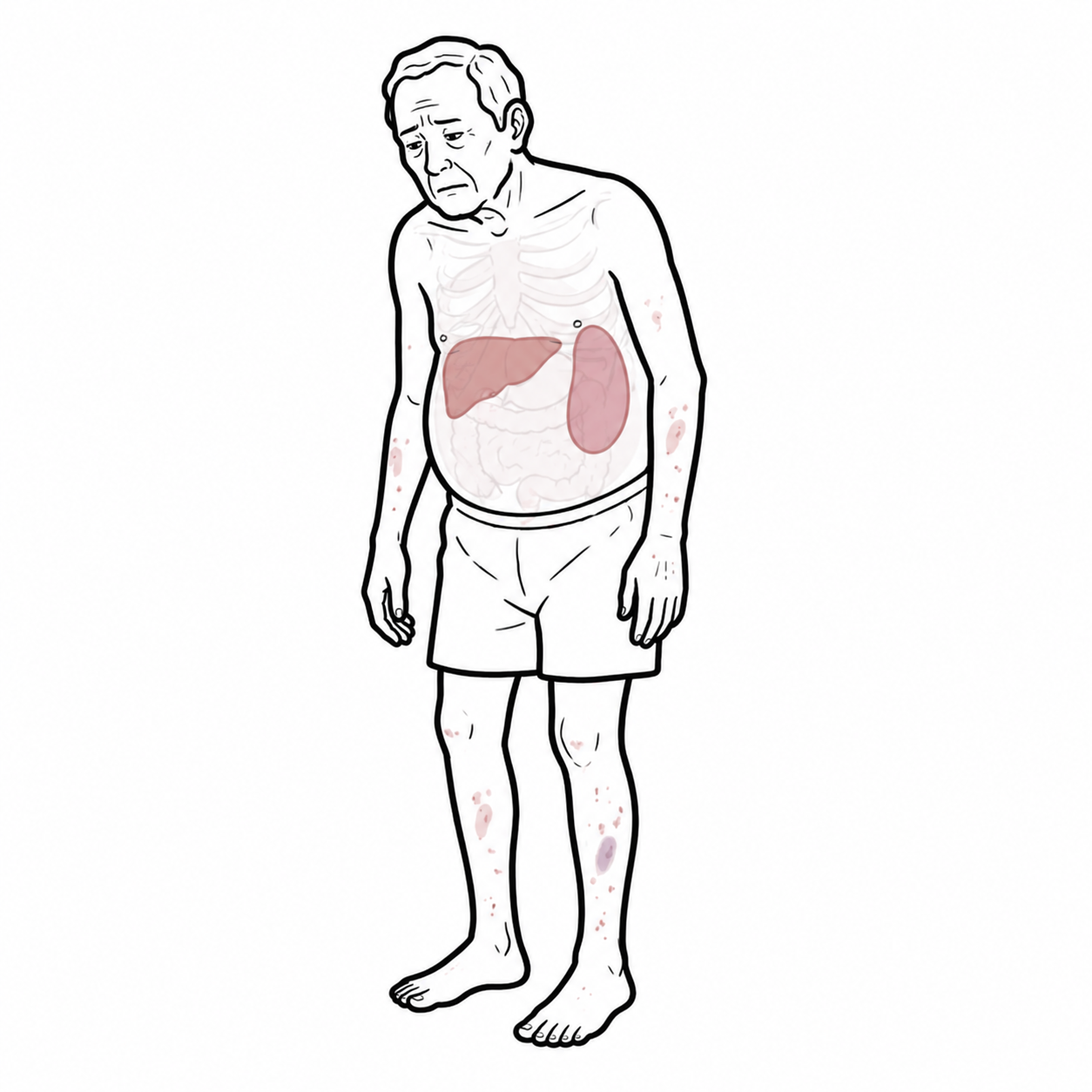
Clinical manifestations of megaloblastic anemia include pallor, tachycardia, weakness, fatigue, and palpitations. The specific mechanism by which vitamin B12deficiency affects the neurologic system is unknown.
There are extensive hepatic stores of vitamin B12. There may be a five- to 10-year delay between the onset of deficiency and the appearance of clinical symptoms.
- Fatigue
- Short of breath
- Headache
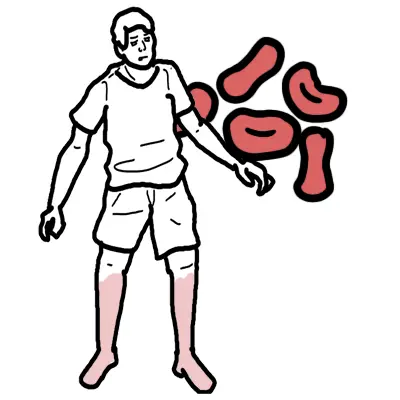
- Pallor, hyperpigmentation
- Muscle Weakness
- Dizziness and Confusion
- Paraesthesia (numbness)
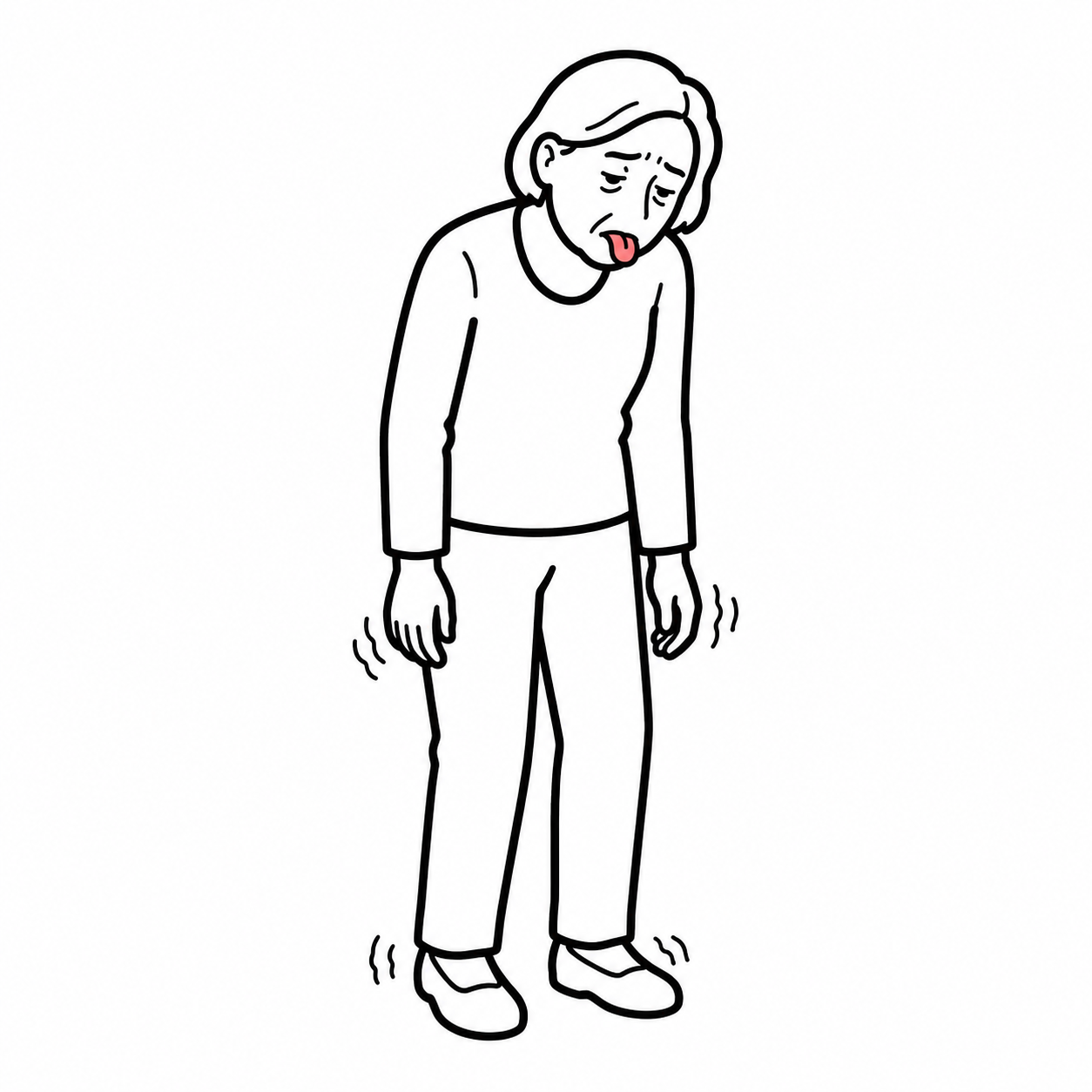
- Ataxia (loss of normal control of body movements)
- Atropic Glosstis (smooth erythematous surface of tongue)
Peripheral neuropathy is the most common symptom of vitamin B12 deficiency. Folate deficiency alone typically has no neurological symptoms.
Differential Diagnosis
| DIFFERENTIAL DIAGNOSIS OF MACROCYTIC ANAEMIA (MACROCYTOSIS) | ||
| Macrocytic Anaemia | Clinical Features | Investigations |
| Vitamin B12 deficiency | paresthesias related to peripheral neuropathy, poor or strict vegan diet, lack of socioeconomic resources, bowel-related symptoms (including diarrhea), or a history of bowel surgery for weight loss. Findings on physical examination may include neurologic signs such as ataxia, decreased proprioception, and vibratory sensation. Patients may also have poor dentition or nonspecific oral stomatitis or glossitis. | Serum Vitamin B12. |
| Alcohol excess | Physical findings consistent with alcoholism include gynecomastia, caput medusae, and jaundice. | The mean corpuscular volume is generally less than 110 fL with chronic alcohol use. Abstinence from alcohol rapidly corrects the elevated mean corpuscular volume |
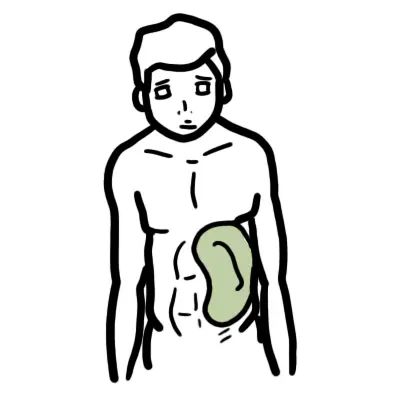
| Reticulocytosis | Family History of haemotological syndromes (sickle cell disease, hereditary spherocytosis, G6P dehydrogenase deficiency). Examination may reveal hepatosplenomegaly in hemolysis or other physical manifestations of blood loss (e.g., conjunctiva, mucosal pallor | Peripheral smear will reveal evidence of hemolyzed RBCs (e.g., bite cells, helmet cells) |
| Myeloproliferative disorders | Splenomegaly, hepatomegaly, fatigue | Bone marrow biopsy is required to establish this diagnosis |
| Hypothyroidism | Mental sluggishness, obese, fatigue, sleepy | Thyroid function test |
| Folate deficiency | Serum folate levels are not useful. RBC folate levels is more accurate. | |
In differentiating the cause of megaloblastic anemia, a methylmalonic acid level that is within normal range also points toward a diagnosis of folate deficiency, especially if the serum vitamin B12 level is within the normal range. Note that homocysteine levels will be elevated with vitamin B12and folate deficiencies.
Investigations
Both the clinical recognition of vitamin B12 deficiency and confirmation of the diagnosis by means of testing can be difficult.
- FBC
- Blood smear
- Macrocytic anaemia
- Hypersegmented neutrophils
- Serum vitamin B12 level
- Serum folate
- Methylmalonic acid – more sensitive and specific for the diagnosis.
- Homocysteine
- Anti–intrinsic factor antibodies (pernicious anaemia)
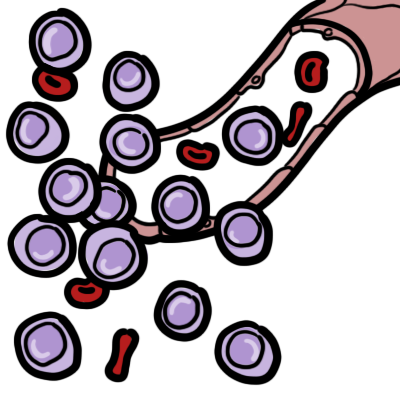
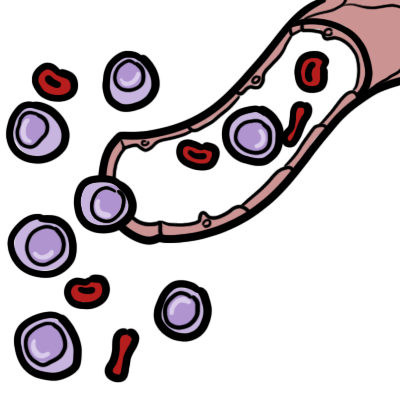
Classic hematologic expression of vitamin B12 deficiency is a megaloblastic macrocytic anemia characterized by an elevated mean corpuscular volume and mean corpuscular hemoglobin, and a peripheral smear containing macroovalocytes and hypersegmented neutrophils.
Serum vitamin B12 levels can be normal even in vitamin B12 deficiency. This is because during periods of stress, the body will produce more transcobalamin (carrier protein for VB12). Measuring methylmalonic acid is thus more sensitive.
Treatment
- High-dose oral Vitamin B12 supplements
- Parenteral cyanocobalamin or hydroxocobalamin
- Multivitamins – for vegans
Complications and Prognosis
Exclusively breastfed children of mothers with vitamin B12 deficiency are at increased risk of failure to thrive, hypotonia, ataxia, developmental delays, anemia, and general weakness.
- Neurolgical deficits
- Haemotological deficits
- Gastric cancer (pernicious anaemia)
Vitamin B12 deficiency can cause devastating neurological disease and severe haematological disorders. Early diagnosis and prompt treatment may reverse neurological disease. Unfortunately, many cases are irreversible and clinical disease may not respond to adequate therapy.
Pernicious Anaemia
Overview
Pernicious Anaemia is a condition where there is lack of intrisinc factor, a glycoprotein responsible for the absorption of Vitamin B12. Vitamin B12 (Cobalamin) is an essential vitamin responsible for many physiological process in our body. Vitamin B12 deficiency causes megaloblastic anaemia and maybe accompanied by neurological abnormalities.
Clinical Presentation
- Fatigue
- Short of breath
- Headache
- Pallor
- Muscle Weakness
- Dizziness and Confusion
- Paraesthesia (numbness)
- Ataxia (loss of normal control of body movements)
- Atropic Glosstis (smooth erythematous surface of tongue)
Differential Diagnosis
- Anaemia:
- Iron Deficiency Anaemia
- Folate (Vitamin B9) Deficiency Anaemia
- Thalassemia
- Aplastic Anaemia
- Neurological:
- Peripheral Neuropathy
- Diabetic Neuropathy
- Multiple Sclerosis
- Gastrointestinal Disease:
- Inflammatory Bowel Disease
- Celiac Disease
- Peptic ulcer Disease
Investigations
- Full blood count: Elevated Mean Cell Volume (MCV) and low haematocrit
- Peripheral blood smear: Megalobastic maturation and hypersegmented neutrophils
- Serum Vitamin B12
- Serum Iron
- Intrinsic factor antibody
- Parietal cell antibody
Aetiology Pernicious Anaemia is associated with the following:
- Autoimmune metaplastic atrophic gastritis (AMAG): AMAG is an inherited autoimmune disease that attacks parietal cells. The immune system targets the Na+/K+ ATPase pump on parietal cells resulting in cell apoptosis. Parietal cells are responsible for secreting acid for digestion and intrinsic factor (IF) for Vitamin B12 absorption. AMAG leads to pernicious anaemia.
- Autoantibody formation against intrinsic factor: Autoantibodies can target IF preventing the binding of IF to Vitamin B12
- Autoantibody formation against intrinsic factor receptors: Autoantibodies can target IF receptors on Ileal cells preventing IF binding to IF receptors.
- Vitamin B12 is responsible for:
- Lack of IF leads to Vitamin B12 malabsorption
- Immune system attacks Parietal cells, IF or IF receptors resulting in IF deficiency
- DNA synthesis
- Healthy Red blood cell production
- Maintaing health nerve cells
- Vitamin B12 deficiency results in: Slow DNA synthesis → Delayed nuclear maturation → Megalobastic erythropoesis → Megalobastic red blood cells → Anaemia
Symptomatic Treatment For patients with pernicious anaemia or malabsorption, lifelong vitamin B12 therapy is indicated.
- Vitamin B12 parenteral injections (cyanocobalamin)
- Vitamin B12 oral supplements
- Neurologist referral may be indicated
Asymptomatic (poor diet, vegan) Treatment
- Regular Vitamin B12 injection
- Multivitamin
Complications
- Infertility
- Gastric Polyps
- Gastric Cancer and Gastric Carcinoid Tumour
- Neurological deficits
Prognosis
Early diagnosis and treatment is important to prevent severe neurological and haematological deficits. Patients usually do well with treatment.
References
BestPractice
Langan, RC., Zawistoski, KJ. (2011). Update on Vitamine B12 Deficiency. American Family Physician. 83 (12). 1425-1430.
Stabler, SP. (2013). Vitamin B12 Deficiency. New England Journal Of Medicine. 368. 149-160.


Members only discussions coming soon…