

Sickle Cell Anaemia
Overview
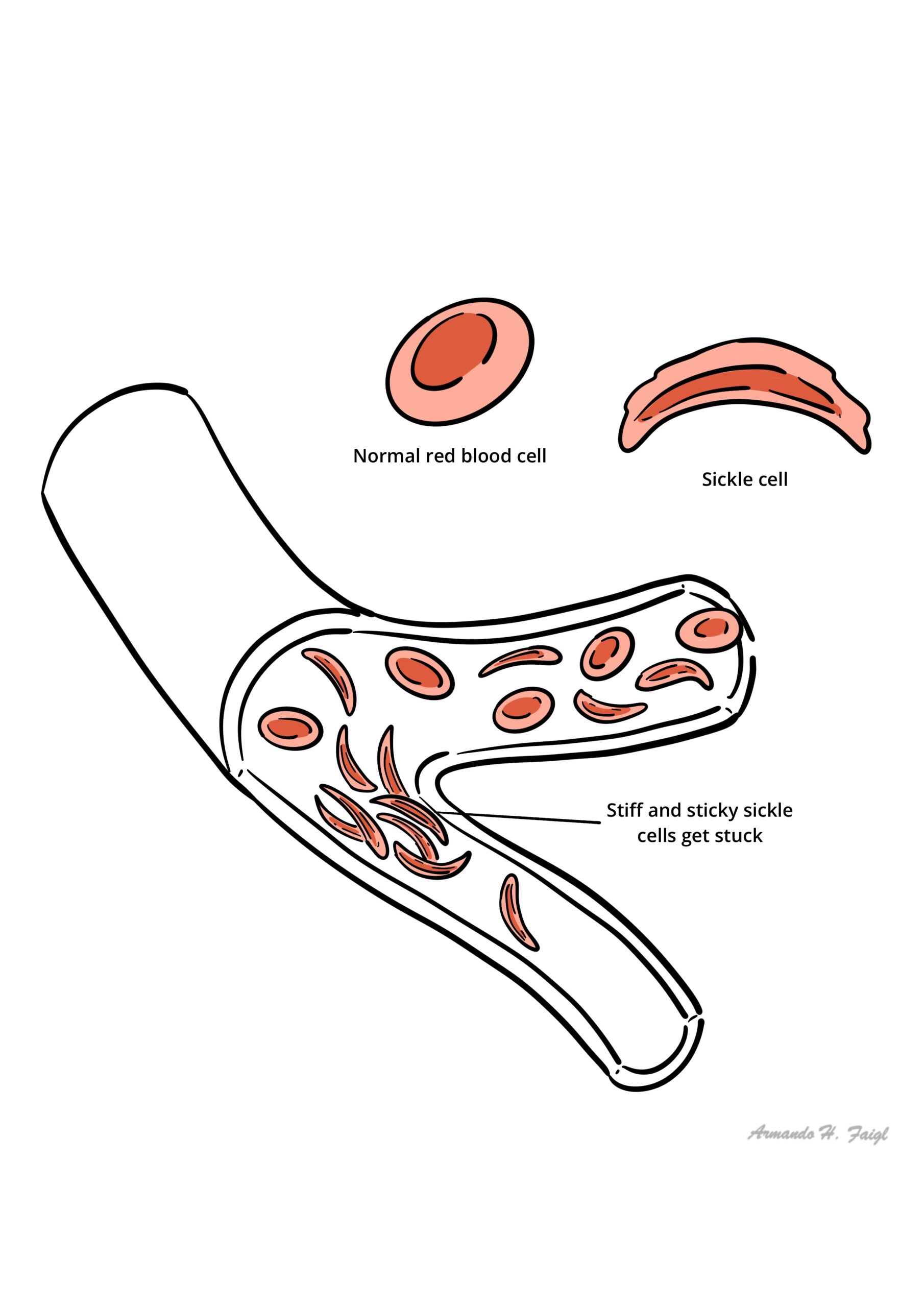
Sickle cell anaemia is an autosomal recessive genetic hemoglobinopathy caused by a single point mutation in the beta-globin gene (HBB) on chromosome 11. This mutation results in a substitution of valine for glutamic acid at the sixth position of the beta-globin chain, producing abnormal hemoglobin S (HbS). Under deoxygenated or stressful physiological conditions, HbS polymerizes, causing erythrocytes to distort into rigid, sickle-shaped cells.
The clinical hallmark of the disease is a dual pathology of chronic hemolytic anemia and microvascular vaso-occlusion. Vaso-occlusive episodes lead to tissue ischemia, severe pain crises, progressive end-organ damage, and functional asplenia, which dramatically increases susceptibility to encapsulated bacterial infections. Sickle cell disease affects millions globally, predominantly individuals of African, Mediterranean, Middle Eastern, and Indian ancestry, where the heterozygous carrier state (sickle cell trait) confers a selective evolutionary advantage against severe Plasmodium falciparum malaria.
Definition
Hemoglobin S (HbS): Abnormal hemoglobin variant produced by a point mutation (GAG to GTG) substituting valine for glutamic acid at position 6 of the beta-globin chain.
Vaso-Occlusive Crisis (VOC): Acute, painful microvascular occlusion caused by sickled erythrocytes adhering to vascular endothelium, leading to tissue ischemia and organ infarction.
Functional Asplenia: Progressive destruction and fibrosis of splenic tissue due to recurrent micro-infarctions (autosplenectomy), resulting in loss of splenic immune filtration by early childhood.
Acute Chest Syndrome (ACS): Life-threatening pulmonary complication characterized by new radiographical lung infiltrates accompanied by fever, chest pain, tachypnea, cough, or hypoxia.
Splenic Sequestration Crisis: Life-threatening acute pooling of a large volume of blood in the spleen, causing rapid splenic enlargement, severe drop in hemoglobin, and hypovolemic shock
Classification
The common variants of sickle cell disease are:
- Sickle cell anaemia (SS disease) is the most common
- Sickle cell trait – causes no disability and protects from malaria except in hypoxia.
- Sickle ß Thalassemia (HbS/ßthal)
- Sickle haemoglobin C disease (HbSC)
Sickle Cell Trait (HbAS) is NOT a form of sickle cell disease. Individuals with sickle cell trait are typically asymptomatic and do not experience vaso-occlusive crises under normal physiological conditions.
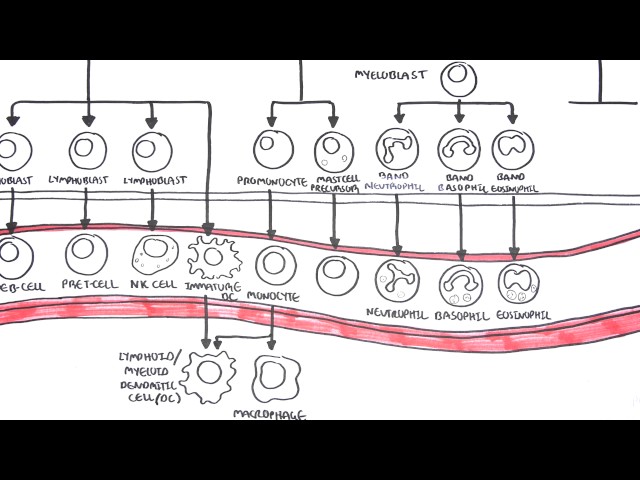
Red Blood Cells Physiology
Aetiology & Risk factors
Aetiology
- Inheritance: Autosomal recessive inheritance. If both parents carry sickle cell trait (HbAS), each offspring has a 25% chance of HbSS, a 50% chance of HbAS, and a 25% chance of normal HbAA.
- Molecular Mutation: Single nucleotide substitution of thymine for adenine (GAG to GTG codon change in HBB gene), replacing hydrophilic glutamic acid with hydrophobic valine at position 6 of the beta-globin subunit.
Triggers for Sickling Crises (flare of sickle cell disease)
- Hypoxia & Altitude: Decreased oxygen tension promotes HbS polymerization.
- Dehydration & Acidosis: Increases intracellular HbS concentration and reduces hemoglobin oxygen affinity.
- Temperature Extremes: Cold exposure induces peripheral vasoconstriction; excessive heat drives dehydration.
- Infection & Stress: Systemic inflammation, fever, and physical or emotional stress.
The single amino acid replacement in HbS is a valine substitution for glutamic acid at position 6 of the beta-globin chain.
Pathophysiology
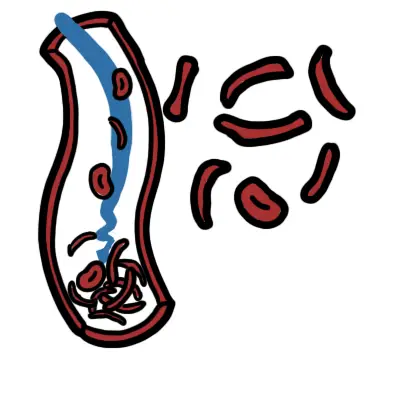
- Polymerization & Membrane Damage: Deoxygenation causes hydrophobic valine residues to assemble into rigid fibrous polymers. Repeated sickling distorts the erythrocyte membrane, causing loss of elasticity, potassium/water leakage, and permanent sickling.
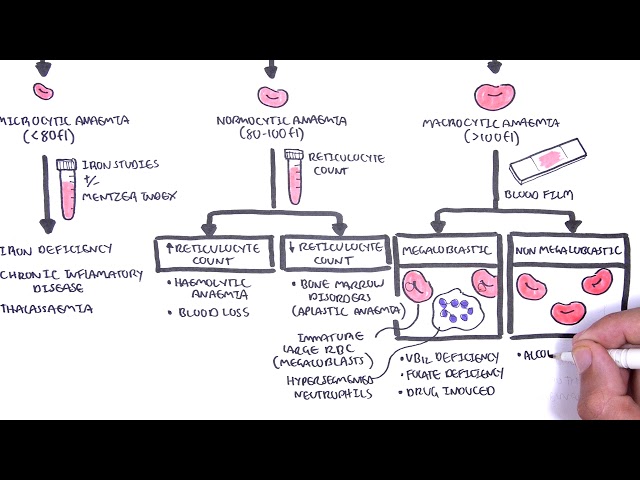
- Hemolysis: Rigid, damaged red blood cells are destroyed intravascularly or cleared by macrophages in the spleen and liver, shortening RBC lifespan from 120 days down to 10–20 days.
- Vaso-Occlusion & Endothelial Dysfunction: Sickled cells exhibit increased expression of adhesion molecules (VCAM-1, P-selectin), sticking to vascular endothelium and trapping leukocytes and platelets.
- Nitric Oxide Depletion: Intravascular hemolysis releases free hemoglobin into plasma, which scavenges nitric oxide (NO). NO depletion drives baseline vasoconstriction, endothelial inflammation, and smooth muscle proliferation.
Free plasma hemoglobin released during intravascular hemolysis scavenges nitric oxide (NO), leading to baseline systemic vasoconstriction, pulmonary hypertension, and endothelial dysfunction.
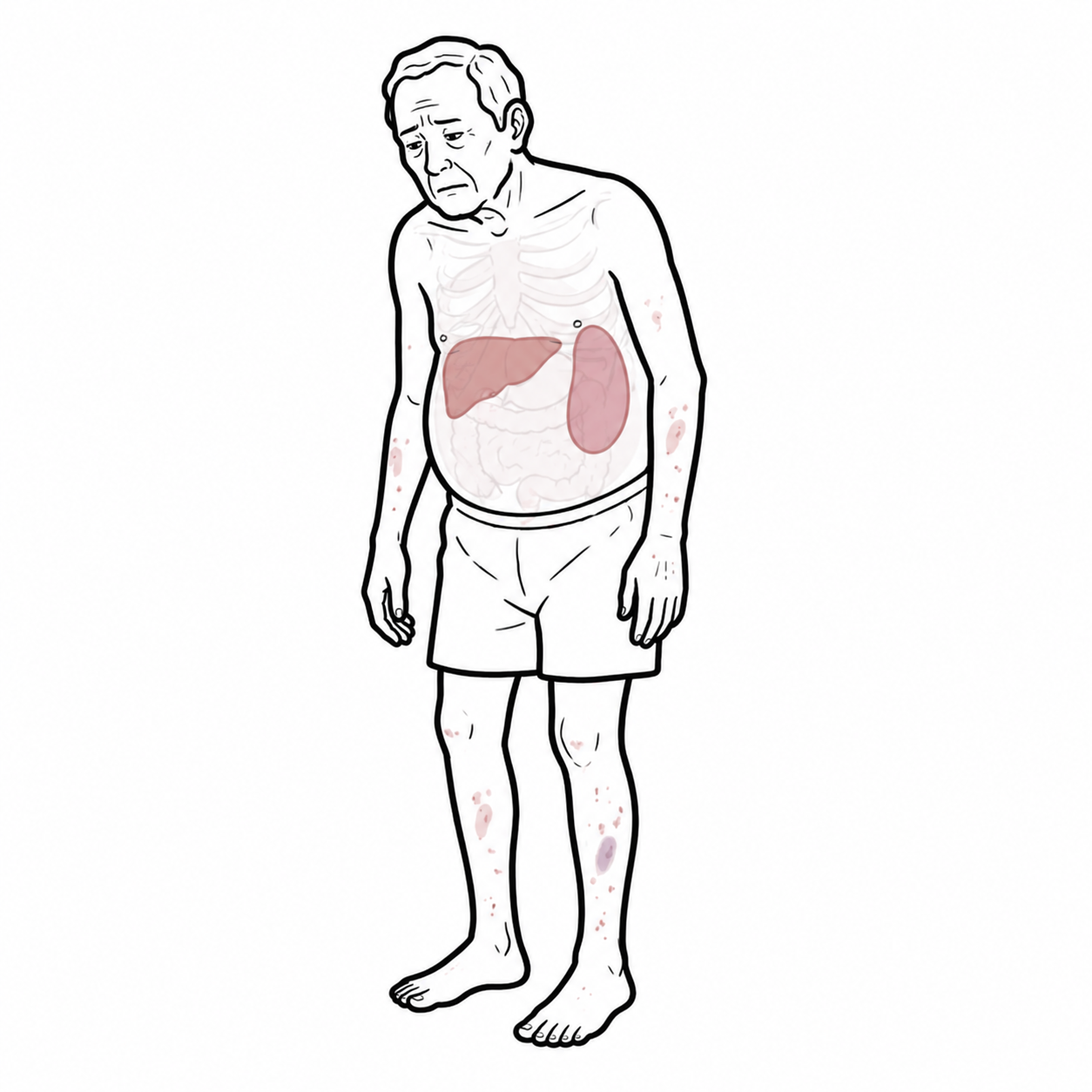
Clinical Manifestation
Newborns are usually asymptomatic because babies still have fetal haemoglobin
- Vaso-occlusive crisis
- Dactylitis (children)
- Mesenteric Ischaemia
- CNS infarction – seziures, stroke, cognitive defects
- Avascular necrosis (neck of femur)
- Leg ulcers
- Priapism
- Fever – infection
- Acute chest syndrome
- a new infiltrate on chest x-ray
- associated with one or more NEW symptoms:
fever, cough, sputum production, dyspnea, or hypoxia.
- Acute splenic sequestration
- Splenomegaly
- Hepatomegaly
- Aplastic crisis – due to parovirus infection, with a sudden reduction in bone marrow production
children typically present with acute dactylitis. Males can present with priapism.
Infectious Manifestations
- Encapsulated Organism Sepsis: Functional asplenia (occurring by age 3 to 5 years due to autosplenectomy) creates extreme vulnerability to fulminant sepsis and meningitis caused by Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae type b.
- Osteomyelitis: High risk of bone infection, characteristically caused by Salmonella species as well as Staphylococcus aureus.
Salmonella is a classic pathognomonic cause of osteomyelitis in patients with Sickle Cell Disease, alongside Staphylococcus aureus.
Investigations
- Hemoglobin Electrophoresis / High-Performance Liquid Chromatography (HPLC): Gold standard diagnostic test.
- In HbSS, demonstrates high HbS (> 80–90%), variable elevated HbF, and 0% normal HbA.
- FBC, reticulocyte count
- Blood film: Demonstrates classic sickle cells (drepanocytes), target cells, nucleated RBCs, and Howell-Jolly bodies (nuclear remnants indicating functional asplenia).
- Sickle Solubility Test (Sickledex)
- Rapid screening test confirming the presence of HbS
- Cannot distinguish between sickle cell trait (HbAS) and disease (HbSS)
Howell-Jolly bodies (nuclear remnants in circulating RBCs) on a peripheral blood smear indicate functional asplenia resulting from auto-infarction of the spleen.
Sickle cell trait have normal blood smear, sickle cell anaemia does not!
Target cells are found in Thalassaemia too.
Sickle solubility test is where a mixture of Hb S in a reducing solution such as sodium dithionite gives a turbid appearance because of precipitation of Hb S, whereas normal Hb gives a clear solution.
Treatment
Disease-Modifying Pharmacotherapy
- Hydroxyurea (First-Line): Ribonucleotide reductase inhibitor that increases fetal hemoglobin (HbF) levels, reduces HbS polymerization, decreases vaso-occlusive crisis frequency, and lowers incidence of Acute Chest Syndrome.
- L-Glutamine: Reduces oxidative stress in sickled erythrocytes.
- Voxelotor: HbS polymerization inhibitor that binds to HbS and stabilizes the oxygenated state.
- Crizanlizumab: Anti-P-selectin monoclonal antibody that inhibits cell-cell adhesion and reduces vaso-occlusive crisis frequency.
Hydroxyurea for prophylaxis of recurrent sickle cell crisis. Eventually person will need regular vaccination because of spleen problems.
Infection Prevention & Prophylaxis
- Prophylactic Penicillin: Daily oral Penicillin V starting from birth or diagnosis until at least age 5 years to prevent fatal pneumococcal sepsis.
- Immunization Schedule: Complete routine childhood vaccines plus additional pneumococcal (PCV20 / PPSV23), meningococcal, and annual influenza vaccines.
Management of Acute Vaso-Occlusive Crisis
- Analgesia: Immediate, aggressive administration of parenteral opioids (e.g., IV Morphine) following step-ladder protocols.
- Rehydration & Oxygenation: Hypotonic or isotonic IV fluids to correct dehydration; supplemental oxygen administered ONLY if SpO2 < 95% or patient is hypoxic.
- Empiric Antibiotics: Broad-spectrum IV antibiotics (e.g., Ceftriaxone) for any fever (>= 38.5°C) due to high risk of rapid septic shock.
Transfusion Therapy
- Simple Transfusion: Indicated for acute severe anemia (aplastic crisis, symptomatic sequestration, acute drop in baseline Hb).
- Exchange Transfusion: Replaces HbS blood with normal donor HbA without increasing blood viscosity; indicated for severe Acute Chest Syndrome, acute stroke, or pre-operative optimization (target HbS < 30%).
Curative & Novel Therapies
- Allogeneic Hematopoietic Stem Cell Transplant (HSCT): Main established curative option for select pediatric candidates.
- Gene Therapy (e.g., Casgevy / Exa-cel): Cell-based gene editing therapy using CRISPR-Cas9 to reactivate fetal hemoglobin (HbF) expression.
Routine prophylactic oral Penicillin from infancy through at least age 5 years significantly reduces mortality from pneumococcal sepsis in children with sickle cell disease.
Complications & Prognosis
- Pulmonary hypertension (major determinant of mortality in adults)
- Chronic restrictive lung disease
- Left ventricular diastolic dysfunction.
- Sickle cell nephropathy (initial glomerular hyperfiltration progressing to proteinuria, focal segmental glomerulosclerosis, and ESRD)
- Hyposthenuria (inability to concentrate urine).
- Proliferative sickle retinopathy (sea-fan neovascularization, retinal detachment, vitreous hemorrhage).
- Chronic leg ulcers (medial/lateral malleoli)
- Avascular necrosis of hips/shoulders.
- Life expectancy has improved significantly over recent decades due to newborn screening, prophylactic penicillin, and hydroxyurea.
- Median life expectancy remains reduced compared to the general population (mid-50s in developed nations).
- Leading causes of death in adults include Acute Chest Syndrome, pulmonary hypertension, sudden cardiac death, and end-stage renal failure.
References
- Kato GJ, Piel FB, Reid CD, et al. Sickle cell disease. Nat Rev Dis Primers. 2018;4:18010. doi:10.1038/nrdp.2018.10
- Ware RE, de Montalembert M, Tshilolo L, Abboud MR. Sickle cell disease. Lancet. 2017;390(10091):311-323. doi:10.1016/S0140-6736(17)30193-9
- Yawn BP, Buchanan GR, Afenyi-Annan AN, et al. Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. JAMA. 2014;312(10):1033-1048. doi:10.1001/jama.2014.10517



Members only discussions coming soon…