

Hodgkins Lymphoma
Overview
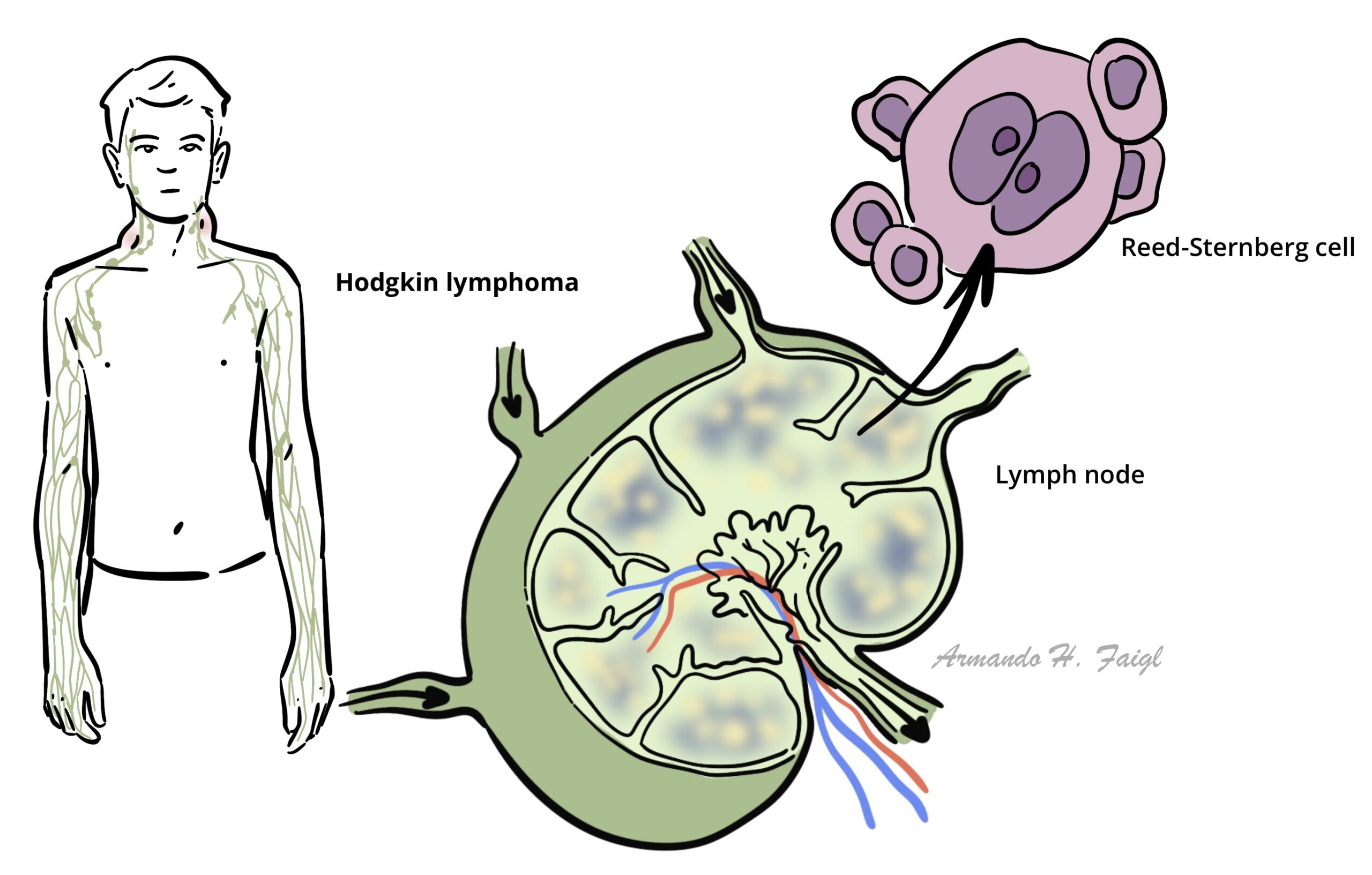
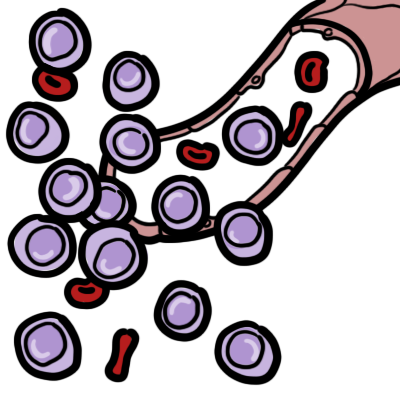
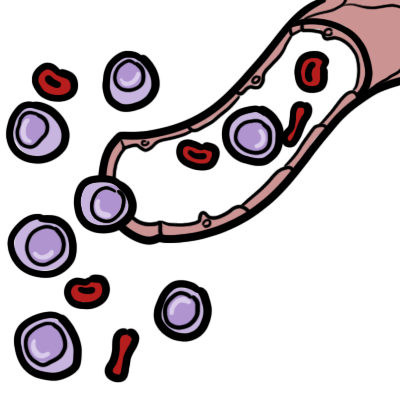
Hodgkin lymphoma (HL) arises from germinal center or post-germinal center B cells. HL has a unique cellular composition, containing a minority of neoplastic cells (Reed-Sternberg cells and their variants) in an inflammatory background.
Reed-Sternberg cell is a characteristic feature of HL.
Epidemiology
- Lymphoma is divided into Hodgkins and Non-Hodgkins
- Hodgkins lymphoma accounts for 10% of all lymphomas
- It has a bimodal age distribution curve – most adolescent
Classification
Classical HL – (90-95% of cases). The tumor cells in this group are derived from germinal center B cells, but typically fail to express many of the genes and gene products that define normal germinal center B cells. Classical HL is further divided into the following subtypes:
- Nodular sclerosis classical HL (NSHL) – (most common)
- Mixed cellularity classical HL (MCHL)
- Lymphocyte rich classical HL (LRHL)
- Lymphocyte depleted classical HL (LDHL)
Nodular lymphocyte predominant HL – The tumor cells in this subtype retain the immunophenotypic features of germinal center B cells.
Risk Factors
- History of EBV infection
- Family history
- Young adults from higher socio-economic status
- Immunosuppression
- Autoimmune disorders
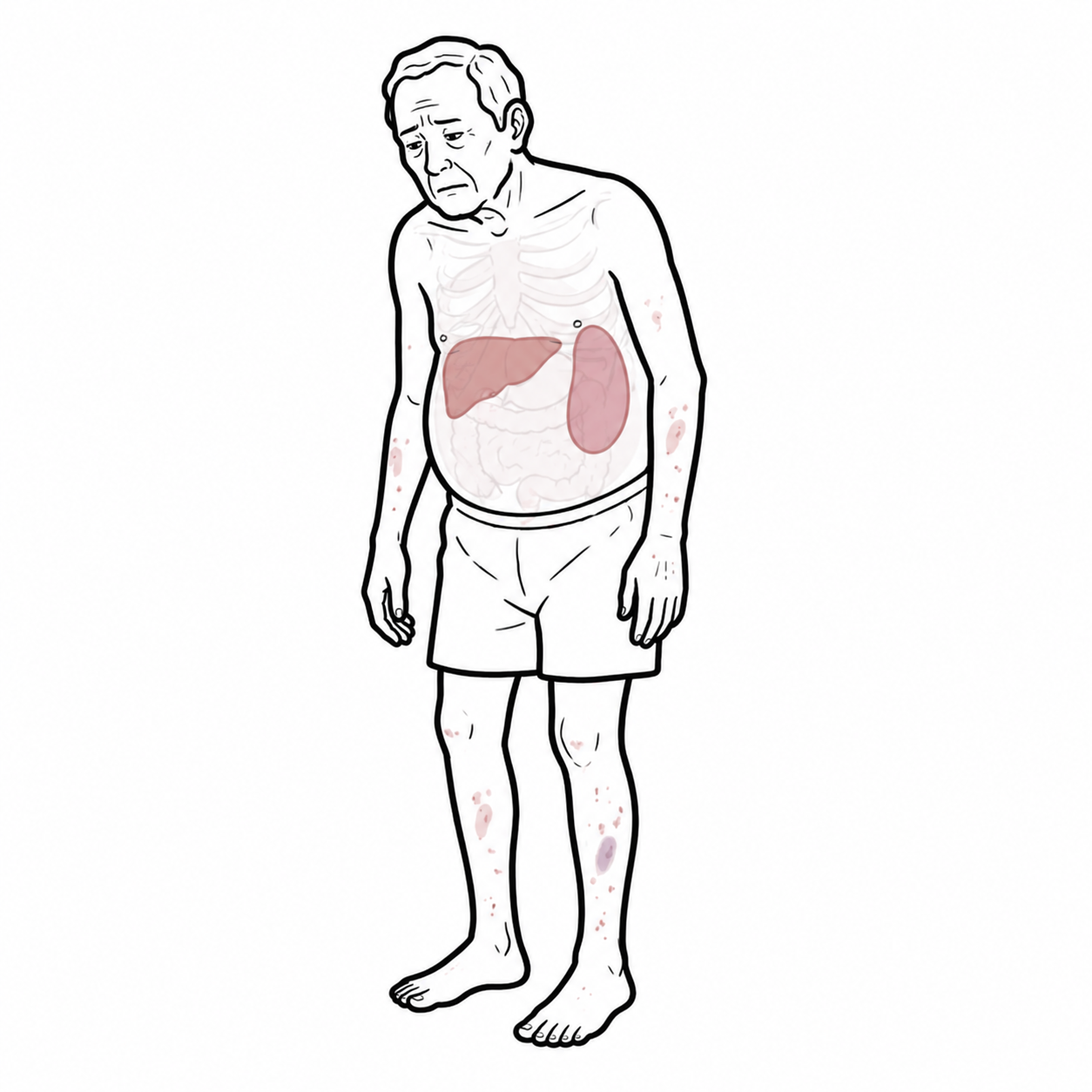
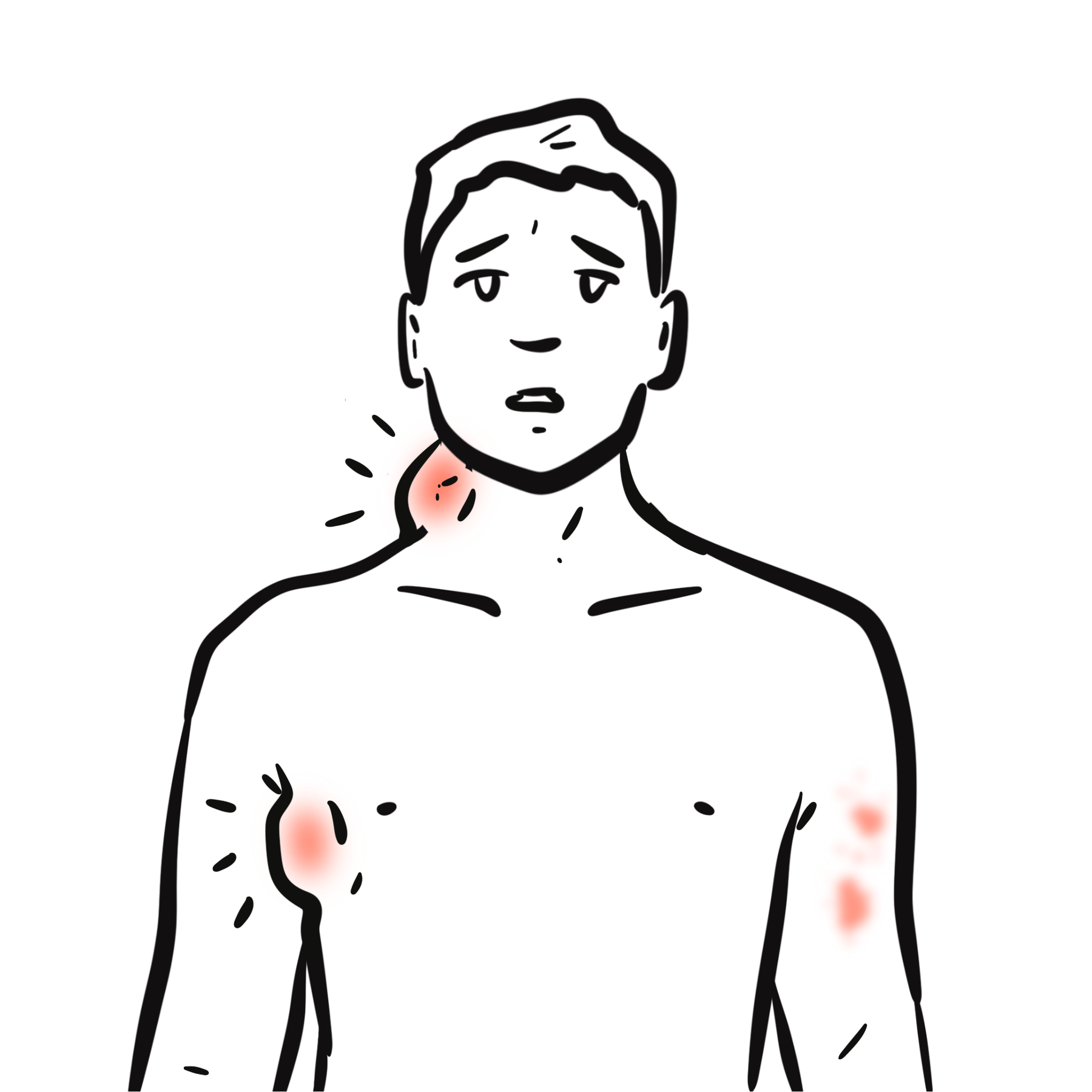
Clinical Manifestations
- Lymphadenopathy – painless, firm cervical or supraclavicular node
- Anterior mediastinal mass
- Cough
- Dyspnoea
- Fever
- Night sweats
- Weight loss
- Anaemia
- Pruritis
Differential Diagnosis
- Non-Hodgkin’s Lymphoma
- Infectious mononucleosis (lymph nodes often tender)
- Reactive lymph nodes
- Infections
- Inflammation (SLE)
Differentials of Lymphadenopathy
- Lymphoma
- Leukaemia
- Metastasis
- Infection
- Connective tissue disease – rheumatoid arthritis, SLE
- Infiltration – sarcoidosis
- Drugs – phenytoin
Investigations
- Full Blood Count
- Low Hb and platelets
- WBC may be high or low
- ESR (Inflammatory marker elevated)
- ↑ Serum Ferritin
- ↑ Serum Copper
- Chest X-ray (Mediastinal mass)
- CT scan – to check for other organ involvement
- PET scan – activity
- Excisional lymph node biopsy (diagnostic for HL and its variants)
- Immunohistochemical studies (to differentiate HL from other lymphomas, classical HL is characteristically CD30 positive and usually CD15 positive)
Diagnosis and staging
- Excisional lymph node biopsy (diagnostic for HL and its variants)
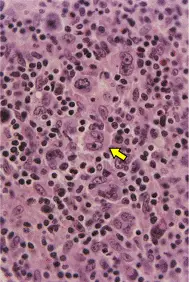
Classic Hodgkins Lymphoma is characterised by the presence of diagnostic Reed-Sternberg cells in an inflammatory back ground.
Ann Arbor staging system
- Single lymph node group
- Multiple lymph node groups on same side of diaphragm
- Multiple lymph node groups on both sides of diaphragm
- Multiple extranodal sites
Pathology
Classical HL is characterised by the the presence of Reed-Sternberg cells in an inflammatory background containing other immune and non-immune cells.
- lymphocytes
- eosinophils
- neutrophils
- macrophages
- plasma cells
- fibroblasts.
Reed Sternberg cells are large cells with abundant, slightly basophilic cytoplasm, bilobed, double, or multiple nuclei, and two or more prominent, eosinophilic, inclusion-like nucleoli.
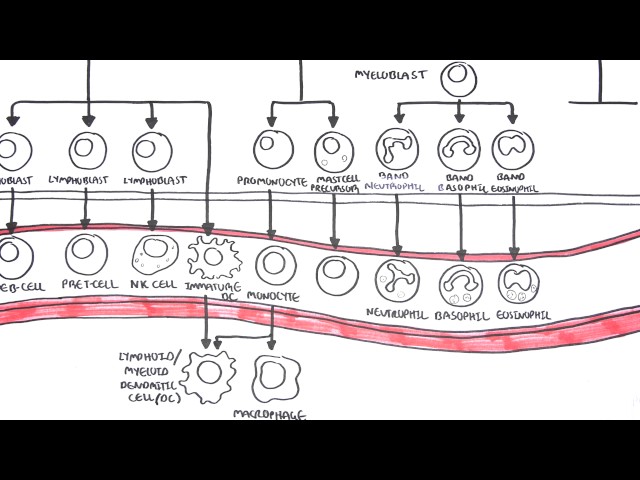
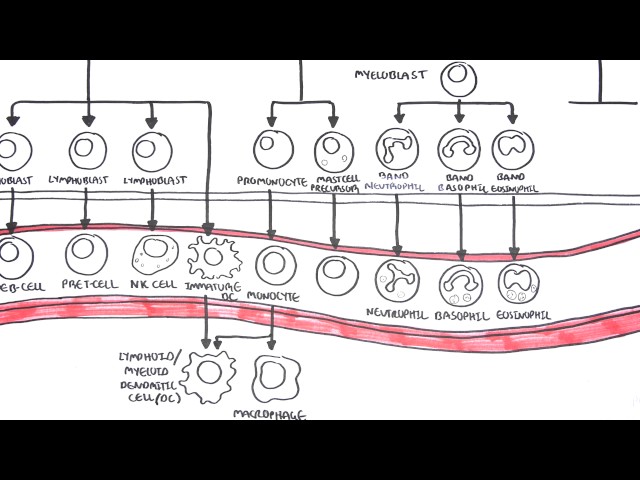
Pathophysioloy
HL is a B-cell malignancy
- B-cells arise from the bone marrow and matures in Germinal Centres within lymph nodes
- B-cells do not undergo proper gene re-arrangments and somatic hypermutation resulting in an abnormal B-cell
- Abnormal B-cells are able to escape apoptosis and can replicate in an uncontrolled manner.
- The abnormal B-cells survive by mimicking cellular receptors that are essential for B-cell growth and survival.
Treatment
Most patients with HL
Chemotherapy (ABVD – doxorubicin, bleomycin, vinblastine, dacarbazine) +/- Radiotherapy
Refractory and relapsing
Chemotherapy +/- radiotherapy + autologous stem cell transplantation is preferred.
Complications and Prognosis
- Radiotherapy related thyroid abnormalities
- Chemotherapy side effects including increase risk of secondary malignancies.
Prognosis
Patients with early stage (stage I-II) HL have a high likelihood of achieving long-term complete remission. A variety of prognostic factors allow for the discrimination of patients with “favourable prognosis” early stage HL and those with “unfavorable prognosis” early stage HL.
- Stage I-II (favourable) 85-90% with chemotherapy followed by low dose radiotherapy.
- Stage I-II (unfavourable) 80-90% with chemotherapy followed by low dose radiotherapy.
Among patients with advanced stage (stage III/IV) HL, prognosis is largely determined by the International Prognostic Score
- Stage III-IV 60-80% with chemotherapy.



Members only discussions coming soon…