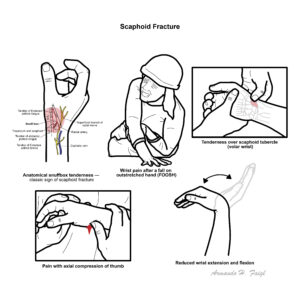
Scaphoid fracture is the most common carpal bone fracture, accounting for ~60–70% of all carpal fractures. It occurs most frequently in young adults (15–40 years) following a fall on the outstretched hand (FOOSH). The scaphoid’s tenuous blood supply predisposes to non-union and avascular necrosis, especially in proximal fractures. Early recognition is essential as delayed or missed diagnosis is common and may lead to long-term disability.
Definition
FOOSH: “Fall On Outstretched Hand,” common mechanism of wrist injuries. Anatomical snuffbox:Depression between tendons of extensor pollicis longus and brevis; tenderness here is pathognomonic for scaphoid fracture. Avascular necrosis (AVN): Bone death due to disruption of blood supply. A common site for avascular necrosis is to the scaphoid bone as well as the hip. Non-union: Failure of bone fragments to heal within expected timeframe.
Anatomy & Physiology
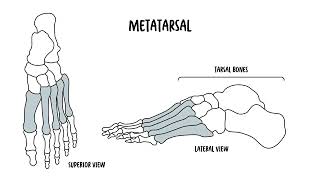
Scaphoid: Boat-shaped carpal bone on radial side of wrist; articulates with radius, trapezium, trapezoid, capitate, lunate.
Blood supply: Retrograde from dorsal carpal branch of radial artery → enters distally → supplies proximal pole last.
Clinical relevance: Proximal fractures at highest risk of AVN due to poor vascularity.
Ibrahim T, Qureshi A, Sutton AJ, et al. Surgical vs non-surgical treatment of acute scaphoid fractures: systematic review and meta-analysis. Cochrane Database Syst Rev. 2008;(4):CD006770.
Buijze GA, Ochtman L, Ring D. Management of scaphoid fractures in adults: what’s new? Injury. 2010;41(11):1120–8.










Discussion