

Testicular Torsion

Overview
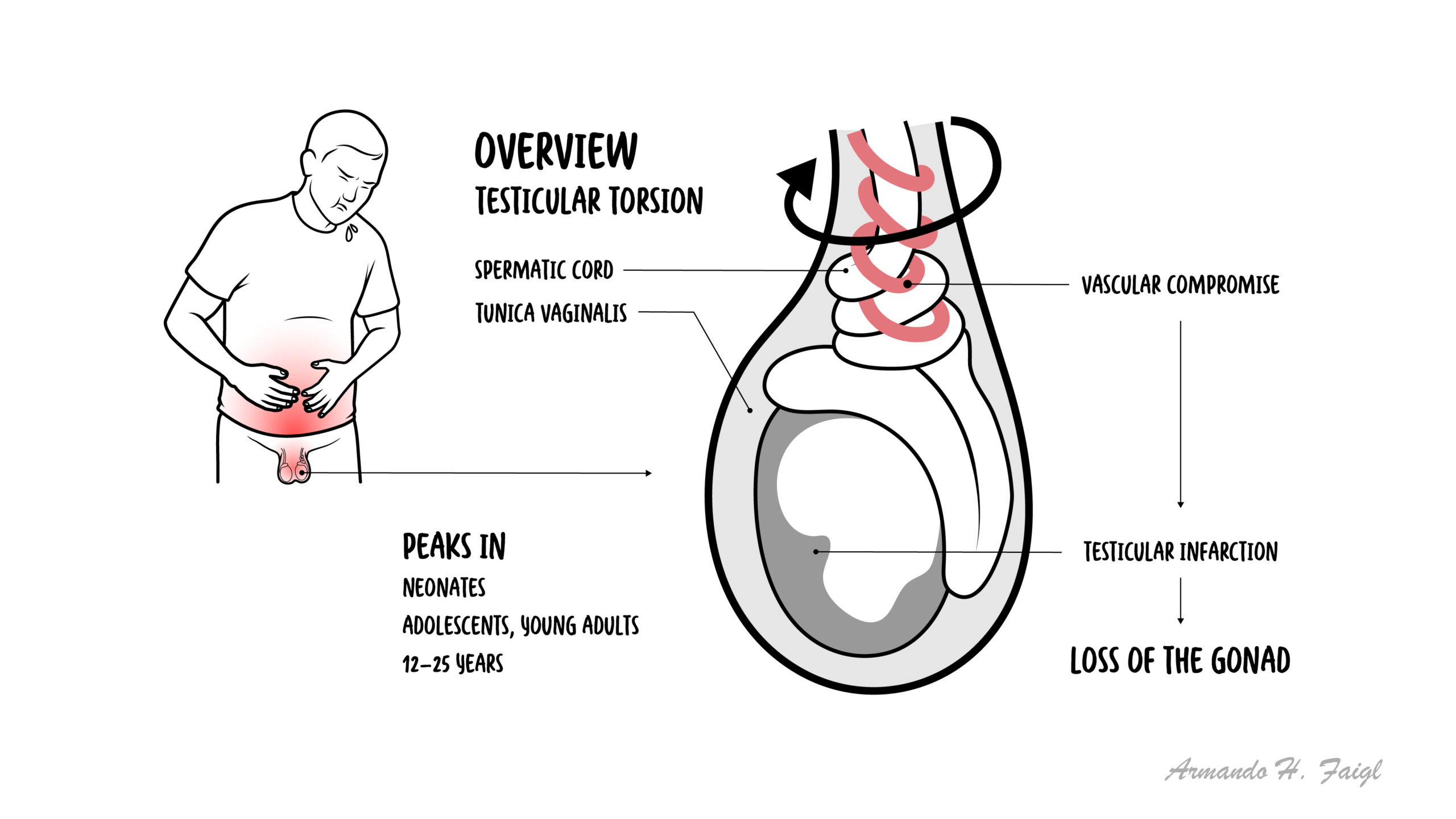
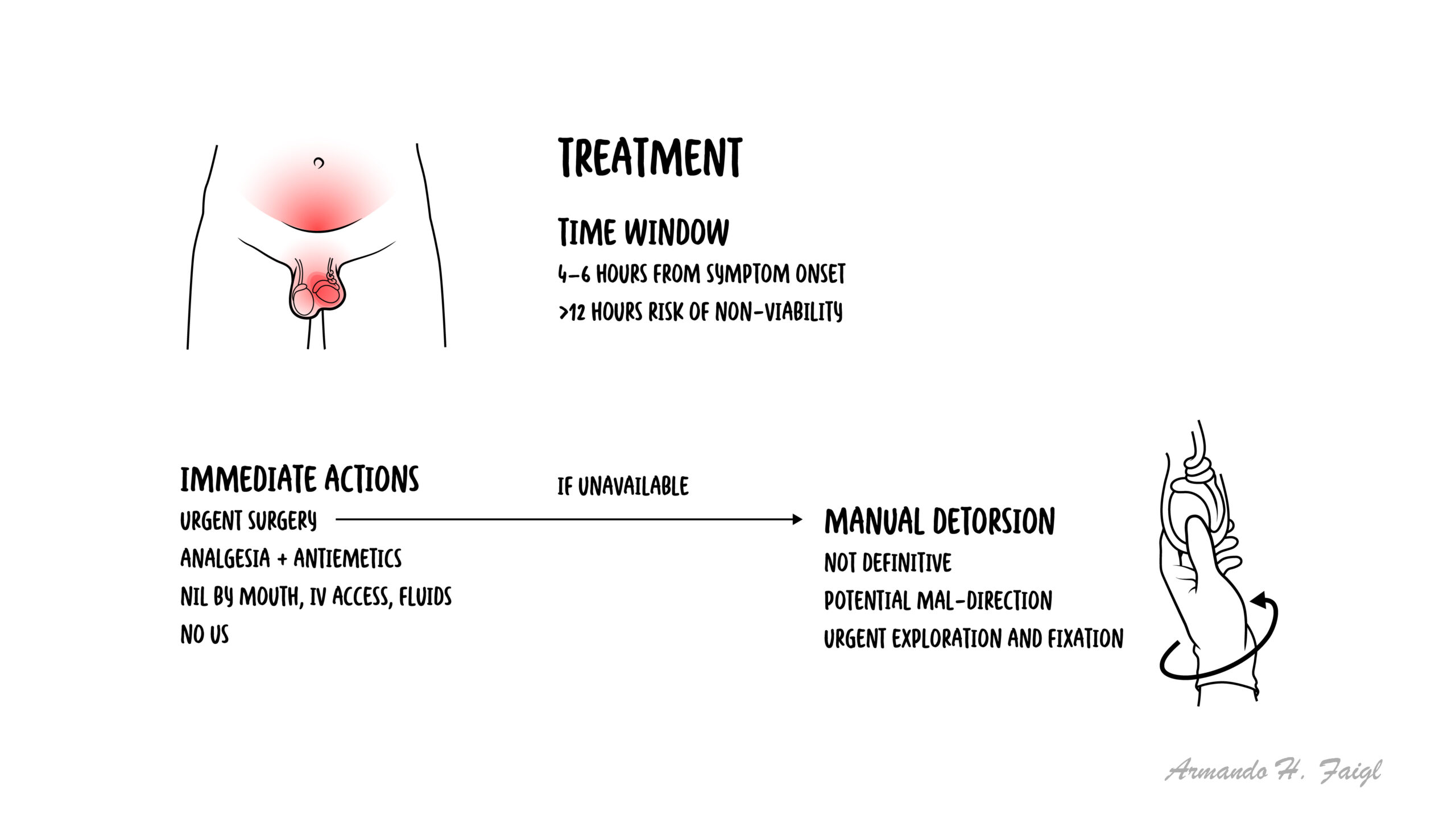
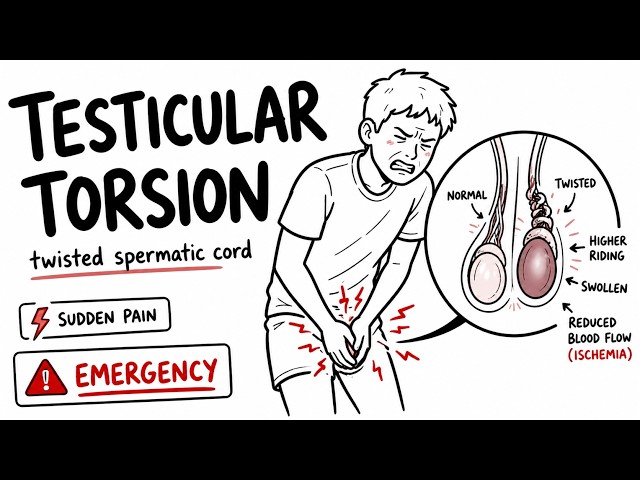
Testicular torsion is a urological emergency caused by twisting of the spermatic cord, leading to acute interruption of blood flow to the testis and rapid ischemia. It most commonly occurs in adolescents (peak 12–18 years) but can occur at any age, including neonates. The incidence is approximately 1 in 4,000 males under 25 years. Early recognition is critical, as testicular viability declines significantly after 6 hours, with high risk of infarction beyond 12 hours. Risk factors include the bell-clapper deformity, trauma, and sudden movement.
Definition
Testicular torsion: Twisting of spermatic cord leading to vascular occlusion.
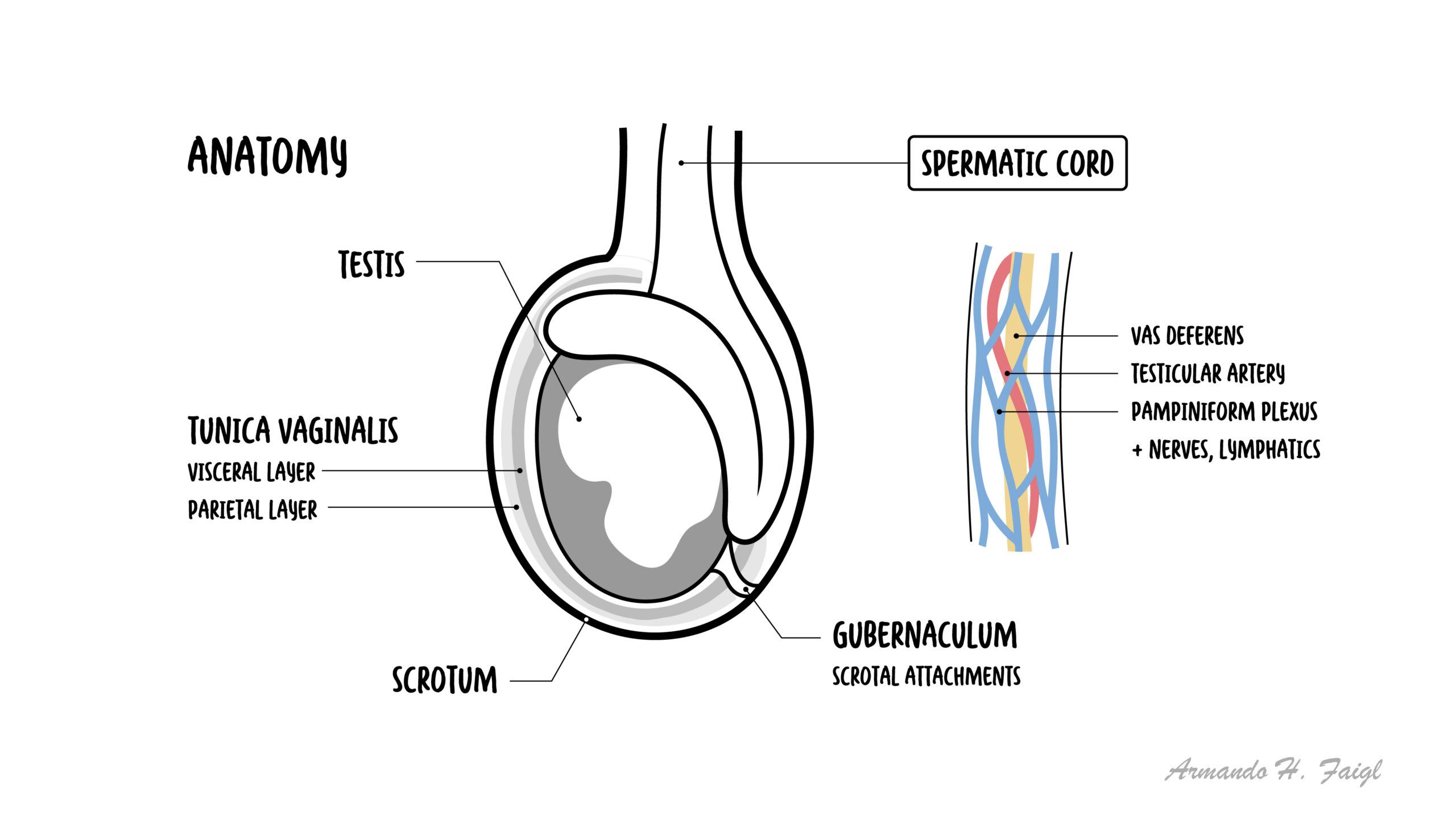
Spermatic cord: Contains vas deferens, testicular artery, veins, nerves.
Ischemia: Reduced blood supply causing tissue injury.
Bell-clapper deformity: Congenital abnormal fixation allowing free testicular rotation.
Anatomy & Physiology
- Testes: Located in scrotum, supplied by testicular artery
- Spermatic cord: Suspends testis and carries vascular supply
- Venous drainage: Pampiniform plexus
- Cremaster muscle: Elevates testis
Aetiology & Risk Factors
Aetiology
- Twisting of spermatic cord
- Often spontaneous
Risk Factors
- Bell-clapper deformity
- Adolescence
- Trauma
- Sudden movement
- Cold temperature (cremasteric contraction)
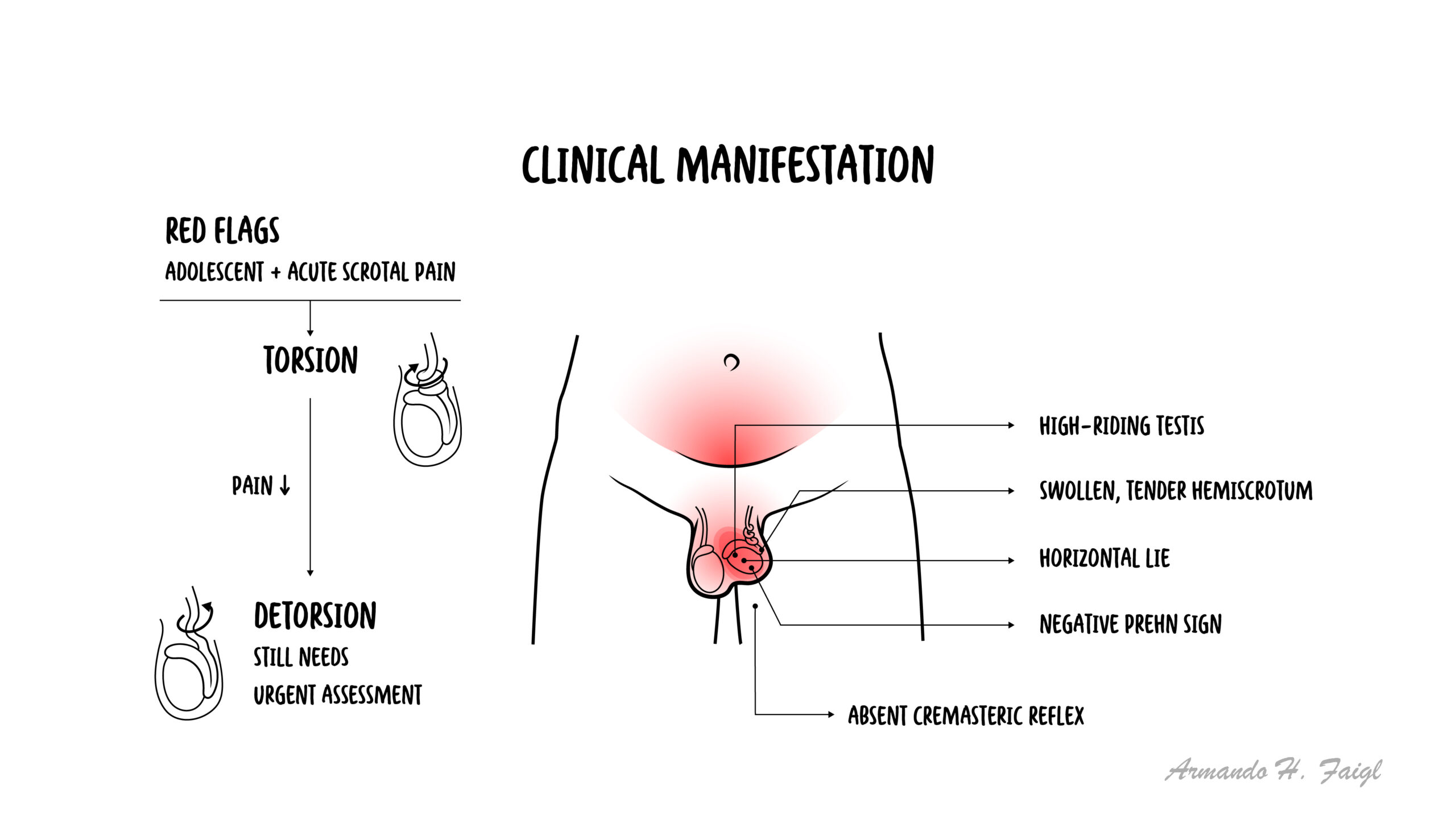
Young male + acute scrotal pain = torsion until proven otherwise.
Pathophysiology
- Twisting of spermatic cord
- Venous obstruction → congestion
- Arterial compromise → ischemia
- Testicular infarction if untreated
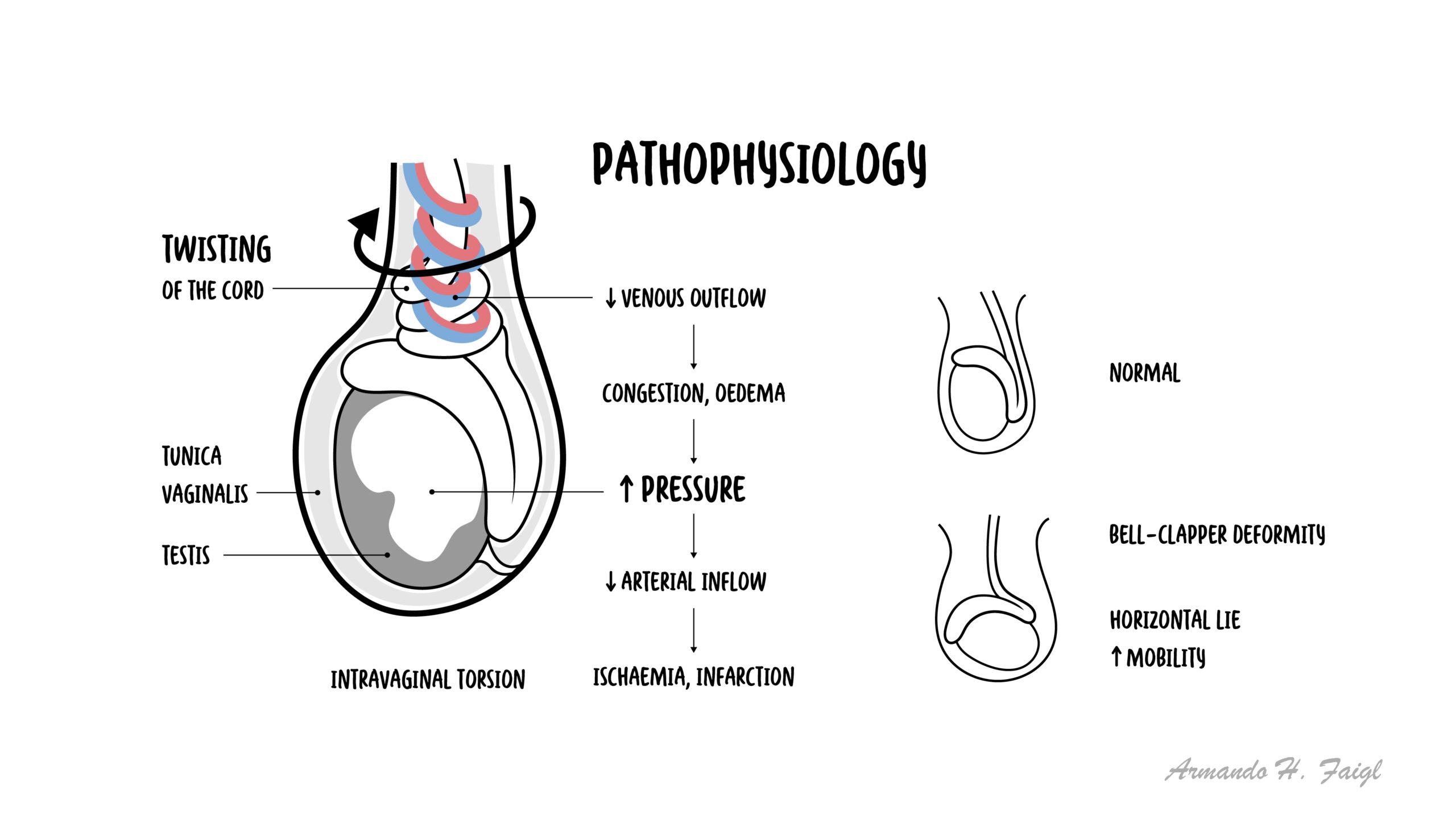
Irreversible damage after ~6 hours.
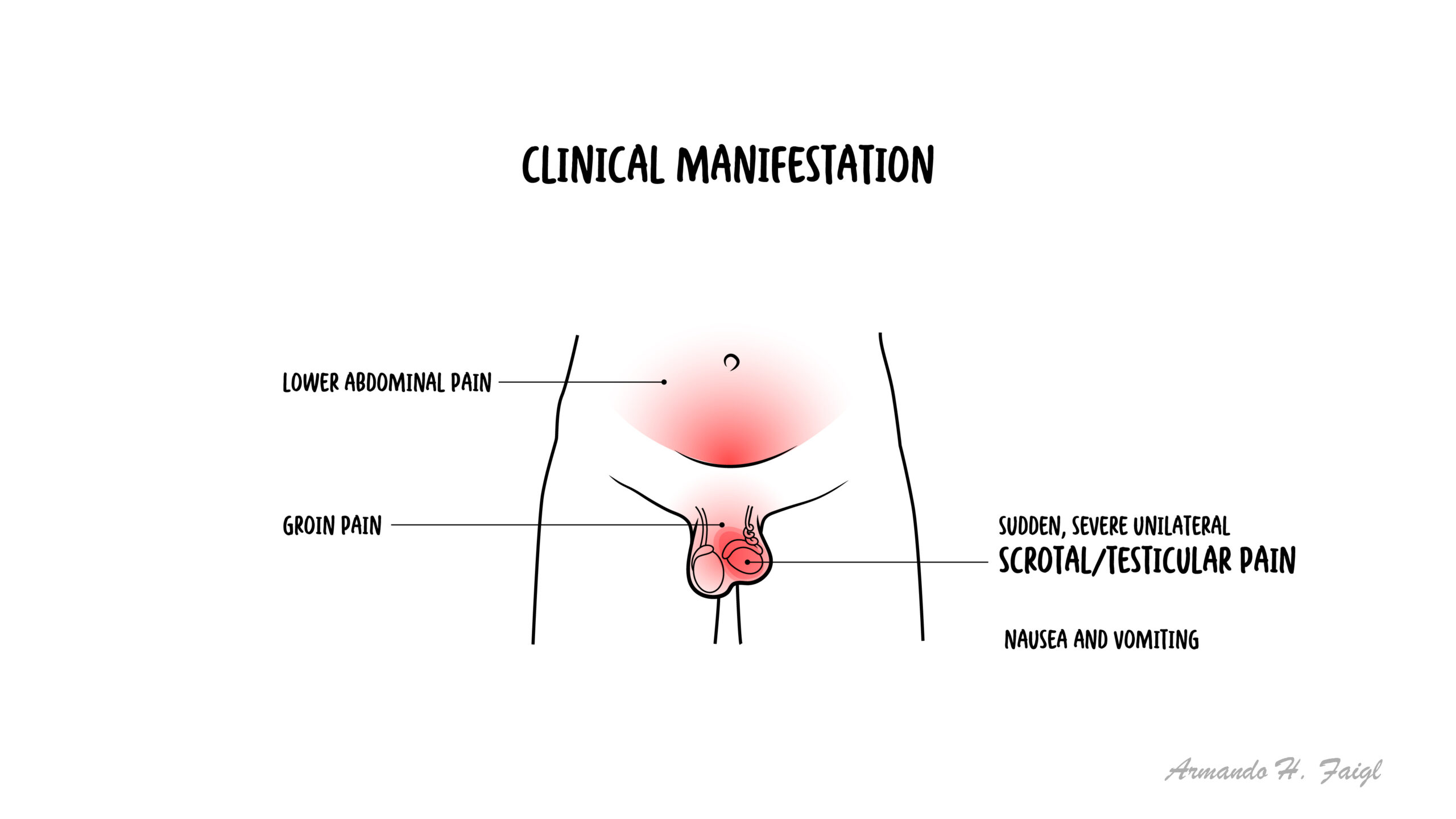
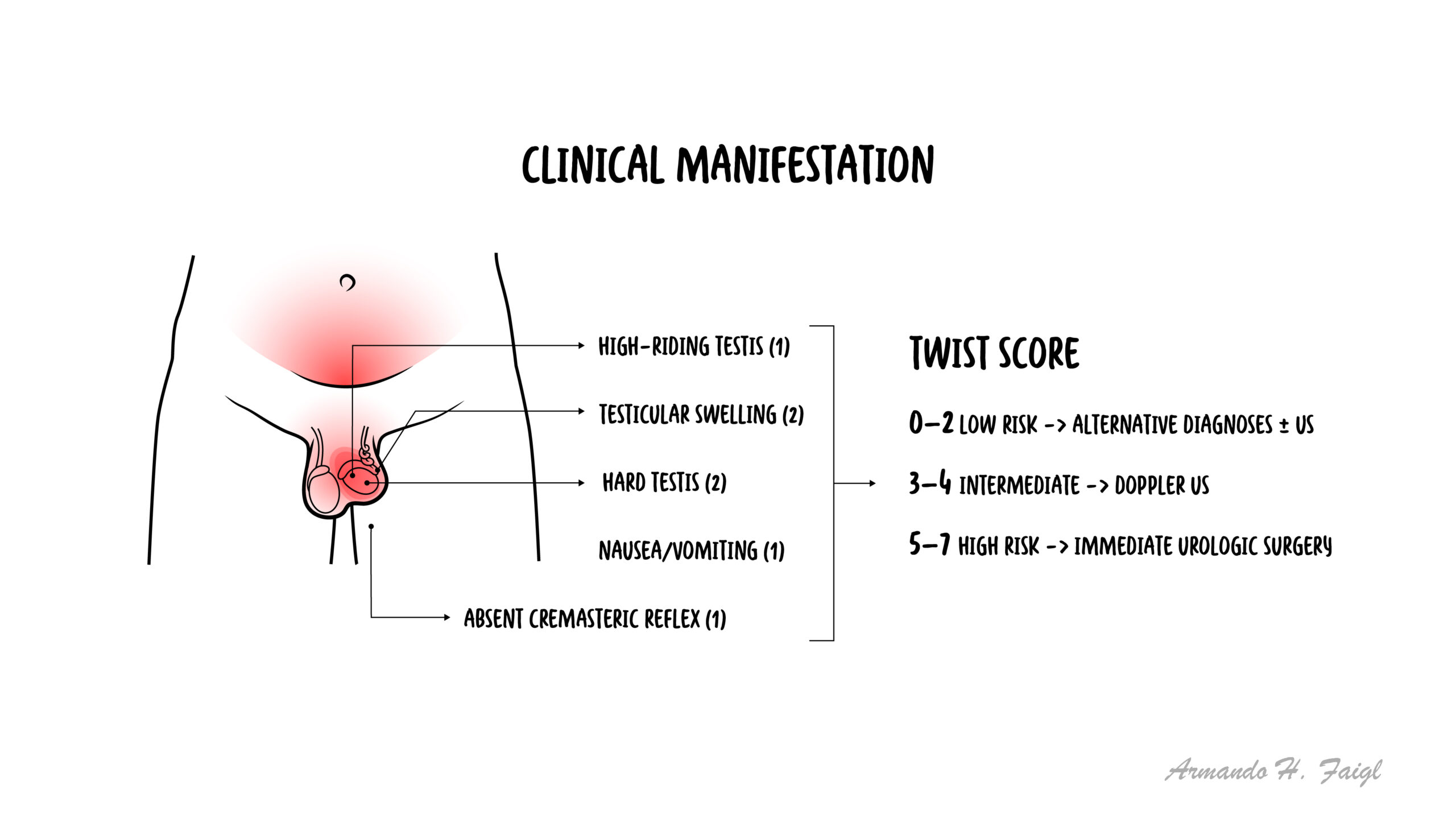
Clinical Manifestations
- Sudden severe unilateral scrotal pain
- Lower abdominal pain
- Nausea and vomiting
- High-riding testis
- Absent cremasteric reflex
- Swollen, tender testis
Diagnosis
- Clinical diagnosis (do not delay surgery)
- Doppler ultrasound (reduced blood flow)
- Urinalysis to exclude infection
Differentials
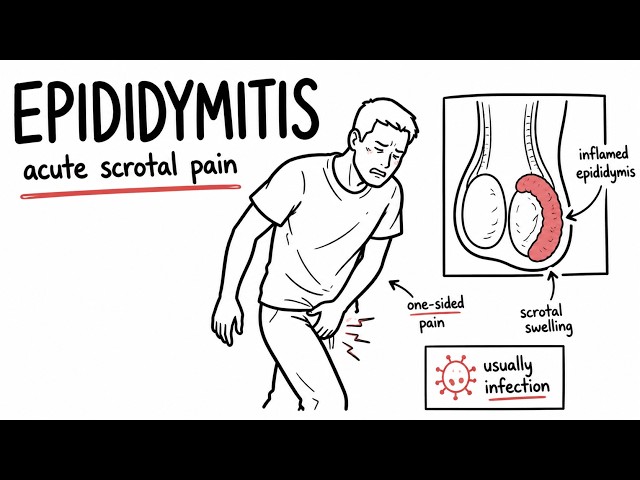
- Epididymitis
- Torsion of appendix testis
- Orchitis
Surgery should not be delayed for imaging.
Classification
- Intravaginal torsion (adolescents)
- Extravaginal torsion (neonates)
Treatment
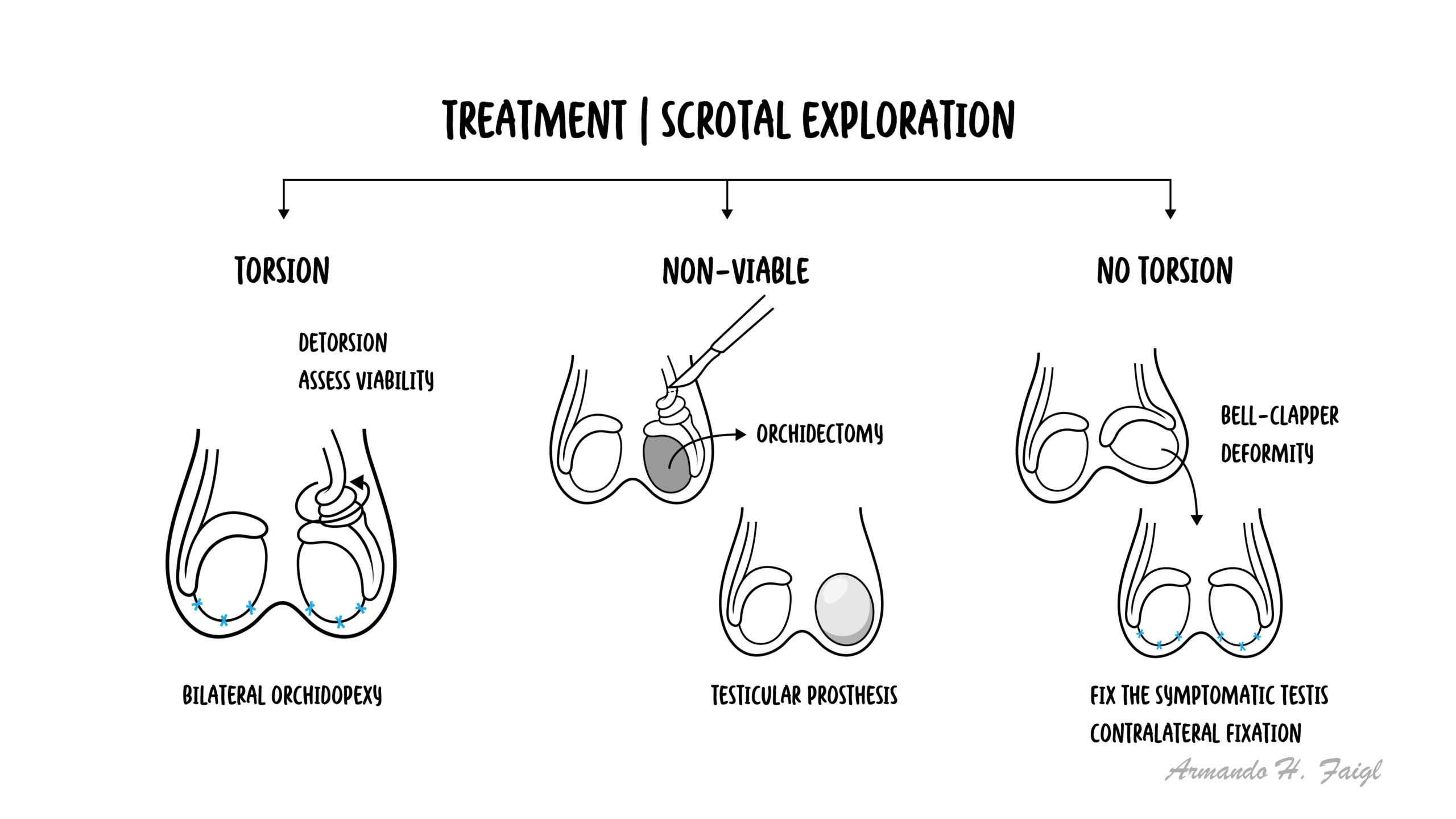
- Emergency surgical detorsion
- Bilateral orchidopexy
- Manual detorsion (temporary if surgery delayed)
Complications & Prognosis
- Testicular infarction
- Infertility
- Testicular atrophy
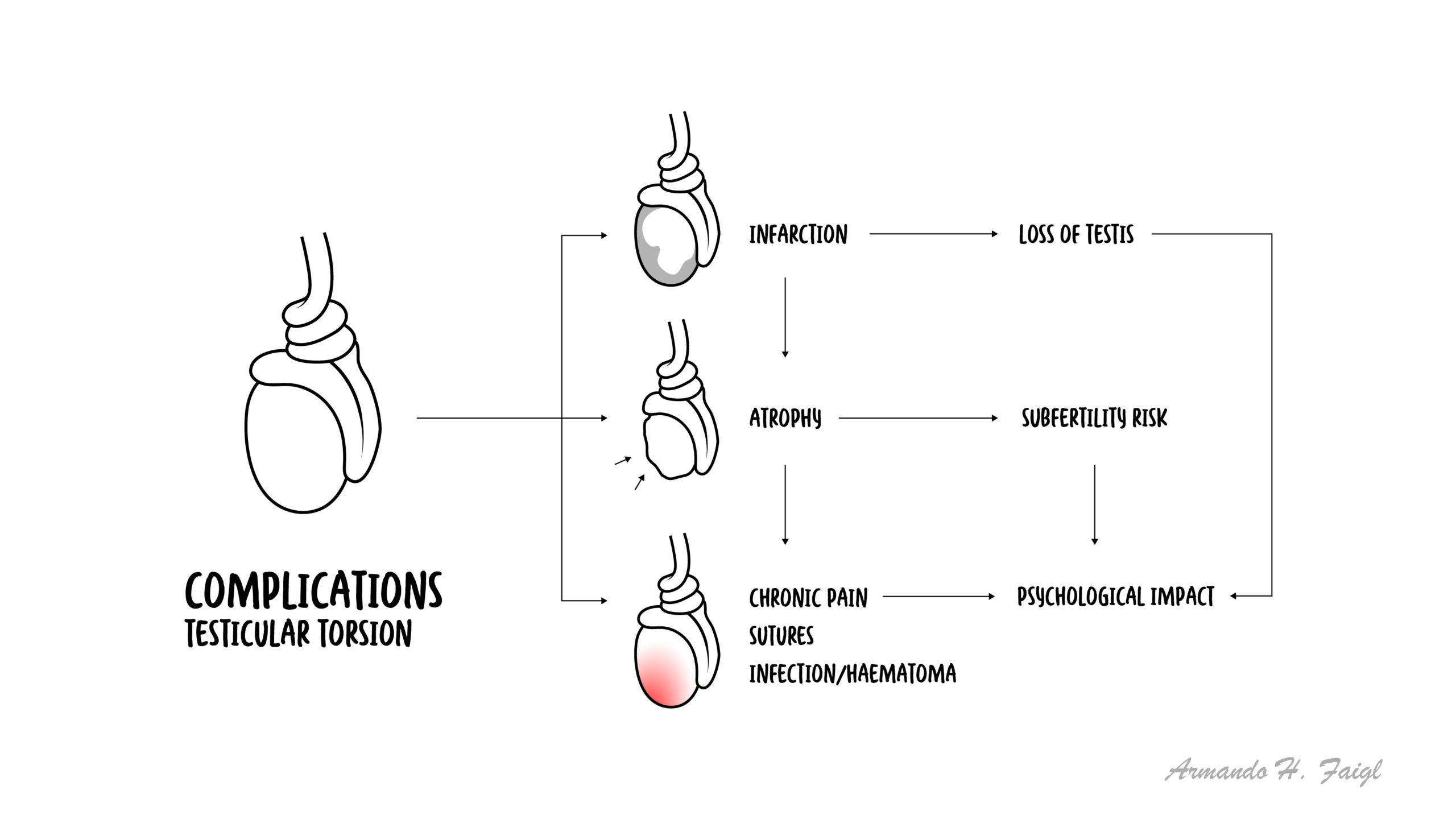
- Good if treated within 6 hours
- Poor if delayed >12 hours
- Salvage rate decreases rapidly with time
References
- Ringdahl E, Teague L. Testicular torsion. Am Fam Physician. 2015.
- NICE Guidelines. Acute scrotal pain.
- European Association of Urology (EAU). Guidelines on testicular torsion.






Members only discussions coming soon…