

Pre-operative Care

Overview
Definition
Perioperative Management refers to the period of time extending from the day prior to surgical intervention to several days after said intervention. It consists of the preoperative, intraoperative and postoperative period.
- Patient education
- Investigation used at surgery
- Coagulation status (ie. INR <2)
- Imaging scans for day of surgery
Pre-operative care
Aims: to provide diagnostic and prognostic information. To ensure the patient understand the nature, aims and expected outcome of surgery. To allay anxiety and pain.
Pre-operative Examination
Assessment of Presenting Illness
Assessment of General Health & Comorbid disease
- General appearance: cachexia, cyanosis, pallor, jaundice
- Height, weight, BMI: Both Malnourished and obese patients are at increased risk from surgical complications.
- Vitals: Heart rate, Blood pressure, respiratory rate, temperature, oxygen saturation
- Cardiovascular Examination
- Respiratory Examination
- Haematological Examination
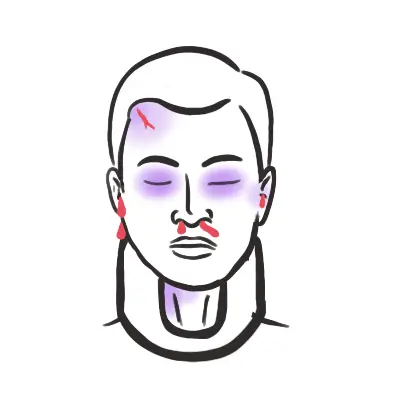
Assessment of Airway – Assesses the likely ease of intubation (LEMON)
- L: Look Externally – Abnormal facies, body habitus, unusual anatomy, facial trauma, facial hair.
- E: Evaluate – 3-3-2 Rule
- 3: Normally a patient should be able to open their mouth to permit 3 fingers. Indicates ease of access to the airway.
- 3: Normally a patient is able to place 3 fingers on the floor of the mandible. indicative of submandibular space.
- 2: Normally a patient is able to place 2 fingers in the superior laryngeal notch. Indicates position of larynx relative to the base of the tongue. If the larynx is two high visualisation of the vocal cords is compromised.
- M: Mallampati Score – Classes signed according to oral cavity & pharynx size. Difficulty of incubation increases from class I to IV.
- O: Obstruction – Upper airway obstruction will impair intubation. Look for evidence of poor dentition (dentures, crowns), supraglottal infection, vocal cord tumours etc.
- N: Neck – Ideally, the patient is placed in the “sniffing position” for intubation. Decreased cervical spine mobility may prevent patients from flexing the head towards the chest.
Assessment of Relevant Anatomical Sites
- Sites for administration of anaesthesia, IV lines, CVP catheters and PA catheters should be identified and examined to ensure they are appropriate.
| Pre-op checklist |
| Blood tests |
| IV cannula |
| ECG + CXR |
| Drug chart |
| Compression stockings |
| Consent |
| Marked site/side |
| Infection risk? |
| Nil by mouth |
Consent
There are four Key Legal requirements of consent (VICS):
- Voluntary: The Patient must be in a position to decide Voluntarily.
- Informed: The patient must be provided with sufficient information. This Patient must be informed of the nature of the condition, the rationale for the proposed treatment, risks (general, specific and material), alternative treatment, time involved, recovery period, follow-up care, costs.
- Capacity: The Patient must have the capacity to understand the procedures implications & make a choice.
- Specific:The Consent must be specific and is only valid in relation to the treatment or procedure for which the patient has been informed and agreed to.
Pre-operative Investigations
Day of Operation
Anaesthetic Bay
- Benzodiazepines given 30min-2hours before surgery to help induce a state of relaxation as well as to decrease the amount of anaesthetic required for induction of anesthesia
Check
- Patient name, date of birth, patient ID (check wrist)
- Site and Side
- Allergies (antibiotic, analgesia)
- Medication (anticoagulation medication stopped – ie warfarin (except for those with prosthetic valves))
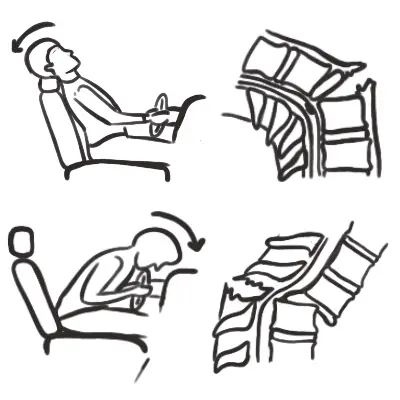
- DVT prophylaxis
- Calf stocking – reduces stasis in infrapopliteal veins by continuous direct compression
- Compression boots – reduces stasis in infrapopliteal veins by intermittently compressing the lower limb veins promoting blood return to the heart.
- LMW heparin 1 hour prior
- Antibiotic prophylaxis
- Given at the same time as induction of anaesthesia.
- Reduce risk of infections post-op
- Selected patients may be continued on antibitic prohylaixis (ie. neutropenic or immunocomprimised)
Other
- Blood or blood product available for selected patient who require transfusion
Patient on wafarin PAP: previous PE, atrial fibrillation, prosthetic valve.
Post-operative care
General
- Check observations chart – vital signs
- Check diabetic charts for blood glucose
- Check catheter bag (ie. urine output, concentration)
- Talk to patient
Examination
- General inspection and listen to patient concerns and questions
- Listen chest, move limbs,
- Check wound and surrounding structures (do not remove dressing)
- DVT prophylaxis (ie, calf pressure)
- Bowel movement
Investigations
- Blood tests: Full blood count, EUC on days 1, 2 and 5
- Anaemia (if low haemoglobin, re-check the next day as it might improve)
- Raised WCC – sepsis
- Monitor INR and clotting daily
- Na+ and K+ to guide choice of fluids
- EUC for patient who have have coexisting cardiac or renal dysfunction
- Investigations and examaination for selected operations
- Orthopaedics – X-ray for prosthesis
- Vascular – 6Ps
- Cardiac – organise a echocardiogram 4-5 days post-op and auscultate daily
- Plastic and reconstructive surgery – check perfusion of flaps
Other
- Patient education
- Rehabilitation plan
More information on Post-operative surgical complications
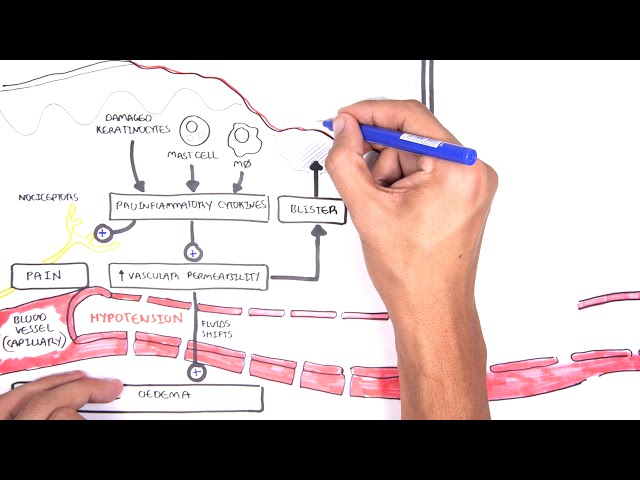
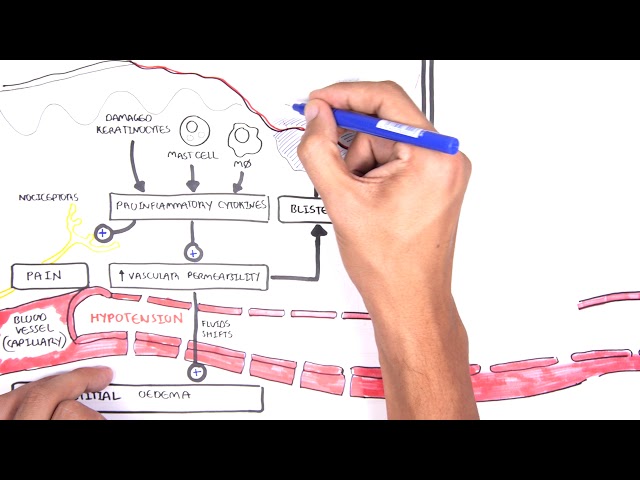
Wound Healing
Definition
Wound:
Acute Wound: is the result of tissue damaged by trauma. This may be deliberate, as in surgical wounds of procedures, or be due to accidents caused by blunt force, projectiles, heat, electricity, chemicals or friction. An acute wound is by definition expected to progress through the phases of normal healing, resulting in the closure of the wound.
Chronic Wound: fails to progress or respond to treatment over the normal expected healing time frame (4 weeks) and becomes “stuck” in the inflammatory phase. Wound chronicity is attributed to the presence of intrinsic and extrinsic factors including medications, poor nutrition, co-morbidities or inappropriate dressing selection
| Stages of Wound healing | Description |
| Haemostasis (immediate) | Vasoconstriction, Platelet aggregation and Coagulation cascade |
| Inflammation (0-3days) | Vasodilation, increased vascular permeability, chemotaxis, immune cells clean up debris and microbes |
| Proliferation (3days – 3weeks) | Fibroblasts migrate into the wound and synthetise collagen. Fibroblasts become myofibroblast which causes wound contraction. Angiogenesis is stimulated by hypoxia and cytokine production |
| Remodelling (3weeks – 1year) | Reorientation and maturation of collagen fibres increases wound strength |
Granulation tissue is the combination of capillary loops and myofibroblasts
Factors affecting wound healing
- Impaired arterial supply or venous drainage
- Excessive movement
- Infection
- Malignancy
- Foreign body and smoking
- Malnutrition
- Immunosuppresive
- Anticancer therapies
- Metabolic (diabetes, uraemia, age)
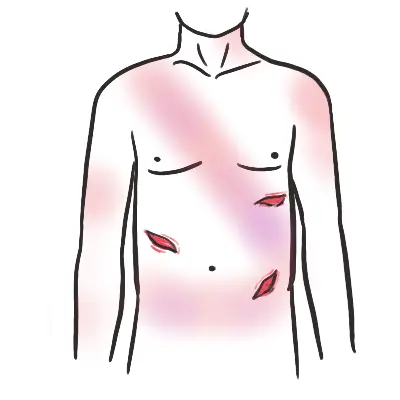
Wound Emergencies
Infection Most caused by patients own flora. Staphylococcus aureus and staphylococcus epidermidis are skin organisms that make up the majority of causes. Escherichia coli and pseudomonas are responsible for many wound infections from opened viscera during surgery.
Dehiscence
Comorbidities and Surgery
Diabetes
Diabetes Mellitus is a Clinical Syndrome characterised by an increase in Plasma Blood Glucose (Hyperglycaemia). Classical symptoms: Polyuria ( Urination), Polydipsia ( Thirst), Polyphagia (hunger). There are 3 main types of Diabetes according to aeitiology:
Approximately half of all diabetics will require surgery at some point during their life, often to manage complications of the disease.
Specific perioperative risks
- Hypoglycemia, hyperglycemia, or ketoacidoiss
- Underlying diabetes-related comorbidites is often unrecognised (ie.mild renal impairment, smal lvessel coronary and cerbrovascular disease, mild autonominc neuropathy with asscoaited rediced cardiovascular homeostasis responses).
- Increased susceptibility to infection, poor wound healing.
- increase susceptibility to skin pressure sore
Management of the diabetic patient
- Inform the anesthetist and other people involved in post operative care (endocrinologisy/diabetic educator)
- Clarify if the patient is orally controlled, insulin-dependent or brittle insulin dependent. As risk of perioperative complication increases with each.
- Diabetics should be first in the operation list
- Check preoperative investigations for signs of underlying combobidities
Ketoacidosis in the perioperative period is associated with a very high morbidity and mortality and should be avoided.
Medication and surgery Depending on the surgery and if it is minor or major surgery oral controlled or insulin control must be stopped on day of surgery. Following surgery it is important to continuously monitor blood glucose level and restart normal medication regime. That is why diabetic patients should be first in line for surgery (for monitoring).
Diabetes Medication plan for the perioperative period.








Members only discussions coming soon…